


ICWA Weekly News 6-25-25
The Department of Health breaks from CDC recommendations; DOH punishes long-term care facilities with rewards; join the team at the Covington Days parade July 19.

Focus on the Washington Department of Health:
DOH Defies HHS Revisions to COVID-19 Shot Recommendations
DOH Punishes Long-Term Care Facilities with Rewards (huh?)
Join ICWA & CHD-WA at the COVINGTON DAYS PARADE July 19th
June 20 Episode of Informed Life Radio – Notes and Links
What is Fluoride? (ICWA, X, Rumble, CHD.TV, CHD-WA)
Guest: Dylan Moore. Drawing from his chemistry background, Dylan Moore of Irida TV differentiates between naturally-occurring fluoride and the industrial byproduct that’s added to municipal water. He discusses the element’s high electronegativity/volatility and potential to disrupt thyroid and calcium functions, and he urges listeners to question the safety, purity, and origin of these additives while suggesting an unexpected approach for the public to advocate for water fluoridation policy change.
Links:
Article: The Manhattan Project's Secret Wartime Conference on Fluoride Toxicity - Fluoride Action Network
Interview [1 hour]: The Fluoride Deception: How a Nuclear Waste Byproduct Made Its Way Into the Nation’s Drinking Water | Democracy Now!
Dylan Moore on Irida TV on these channels: @irida_tv on X, @irida on Gab Social, @iridatv on Telegram, Irida TV on YouTube, and Irida TV on Odysee.
Miami-Dade Mayor Levine Cava vetoes county decision to remove fluoride from water - CBS Miami
Municipal Research and Services Center website “Empowering local governments”
Center For Self Governance – Mark Herr, Washington-based
Local interest: Tacoma Public Utilities “Water Treatment” page, setting forth four additives, including fluoride
DOH Defies HHS Revisions to COVID-19 Shot Recommendations
On May 27, 2025, U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. announced that the Centers for Disease Control and Prevention (CDC) would no longer recommend COVID-19 vaccines for healthy children and healthy pregnant women.

But last Wednesday, Jamilia Sherls, Director of the Office of Immunization for the Washington Department of Health (DOH), sent out a letter that clearly defied Kennedy’s recommendation. Instead of stopping the recommendation of COVID-19 shots for all healthy children and pregnant women, Sherls continued to recommend that all those over six months of age, including pregnant women, get the jabs, as reflected in the start of the letter.
To our health partners,
The Washington State Department of Health continues to recommend everyone 6 months of age and older receive the current COVID-19 vaccine to protect against severe illness. This recommendation includes pregnant people.
This recommendation is informed by the Washington State Vaccine Advisory Committee (VAC). The VAC serves as an advisory body to the Department on appropriate recommendations to control vaccine preventable diseases in Washington state.
Note that this recommendation is “informed” by the VAC. Yet, the VAC most recently met on April 10, well before the CDC vaccine schedule change, so they couldn’t have deliberated on any recommendation – unless they did it outside of the public view. Or they’re just citing a recommendation from a prior quarterly meeting. ICWA has submitted a public records request to learn if /how the VAC was involved.
“The VAC’s most recent "recommendations" are years old. In fact, that page still states that VAC recommends the CDC schedule,” observed ICWA director Lisa Templeton.
Bob Runnells, another director of ICWA, noted that the DOH might now be Kennedy-proofing its recommendations by filtering them through the Washington VAC, not simply passing on those of the CDC’s Advisory Committee on Immunization Practices (ACIP). “The VAC has been pretty useless over the years, and we’ve wondered why it even exists. Now, we see that they may have been maintaining a state-level VAC, mimicking the CDC and FDA review committee structure, for just this situation where they can act like they have better science and judgment and recommend their preferred pro-vax solution,” he said.
Of further note, under “Rationale” on its website, the VAC acts a vaccine marketing promoter for Big Pharma:
Current clinical expertise and recommendations provided by health care providers experienced in relevant fields (vaccinology, preventive medicine, vaccine-preventable disease management, pediatrics, infectious disease, epidemiology, internal medicine, and family medicine) will provide guidance to DOH and inform the strategic implementation of vaccine usage and vaccine administration at the clinical level.
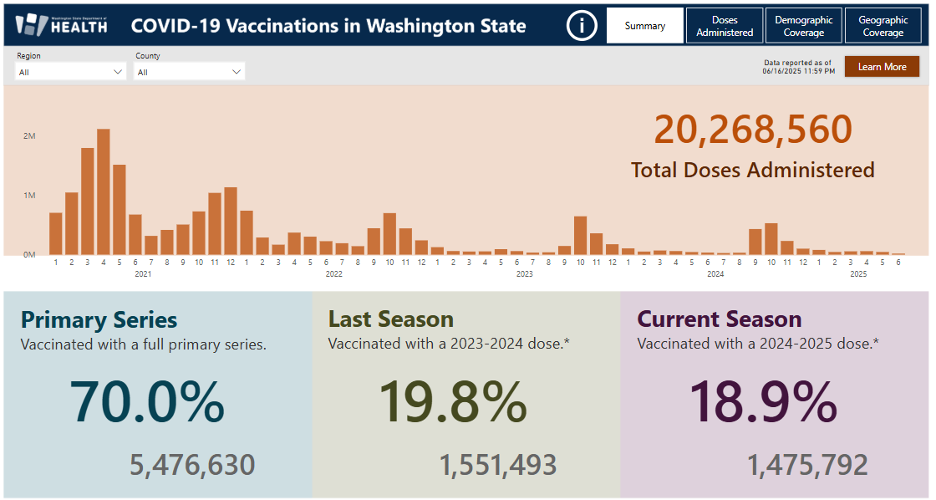
The most recent VAC meeting agenda focused on measles shots. But the group would have been more in keeping with its shot-marketing strategy by addressing the drastic decline in uptake from 70 percent for the primary series to only 18.9 percent for the 2024-2025 booster formulation, as reported by DOH on June 16.
Sherls also writes in her letter, “We are committed to science-based vaccine policy and making sure vaccines stay accessible and equitable for everyone in Washington state. We will promptly share any updates with the public and our partners.”
Conspicuously missing in her letter is any supporting documentation for her “science-based vaccine policy” that all those over six months of age, again including pregnant women, should get the COVID-19 shots. Also absent is an admission that this DOH policy is a departure from the new CDC recommendation. It seems that ICWA members aren’t alone in questioning the CDC—turns out that DOH does, too!
As for the children to whom Kennedy referred, it would be interesting to see the DOH challenge the following CDC citation by Paul Thomas, MD, in Vax Facts at page 171:
As of Nov. 3, 2021, the chance of a child 17 years or younger contracting SARS-CoV-2 and dying from COVID-19 was 1 in 126,000 or 0.0008%.
Citation: Centers for Disease Control and Prevention. 2023. “CDC Web Archive: Weekly Updates by Select Demographic and Geographic Characteristics: Provisional Death Counts for Coronavirus Disease (COVID-19).” cdc.gov. September 27.
Referencing a document from Physicians for Informed Consent, Vax Facts also reports the following vaccinated versus unvaccinated fact concerning children (p. 171):
COVID vaccine trials found no serious COVID illnesses in the unvaccinated children, but for every mild illness in the unvaccinated there were seven severe reactions in the vaccinated children.
Dr. Thomas provides the following six references to support this statement; the DOH and members of the VAC would do well to take the time to study them:
2021. “Pfizer-BioNTech COVID-19 Vaccine: Emergency Use Authorization (EUA) Amendment for an Unapproved Product Review Memorandum—EUA 27034 (Amendment 132).” fda.gov. April 9. https://www.fda.gov/media/148542/download.
2021. “FDA Briefing Document: EUA Amendment Request for Pfizer-BioNTech COVID-19 Vaccine for Use in Children 5 through 11 Years of Age.” fda.gov. October 26. https://www.fda.gov/media/153447/download.
Wallace, Megan. 2021. “ACIP COVID-19 Vaccines Work Group: Grading of Recommendations, Assessment, Development, and Evaluation (GRADE): Pfizer-BioNTech COVID-19 Vaccine.” cdc.gov. May 12. [updated website for the meeting slide deck: https://stacks.cdc.gov/view/cdc/107711/cdc_107711_DS1.pdf]
Centers for Disease Control and Prevention. 2021. “Grading of Recommendations, Assessment, Development, and Evaluation (GRADE): Pfizer-BioNTech COVID-19 Vaccine for Persons Aged 12-15 Years.” cdc.gov. May 14. https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-pfizer-biontech-vaccine-12-15-years.html#table03d. [updated website for the CDC document: https://stacks.cdc.gov/view/cdc/106423/cdc_106423_DS1.pdf]
Pfizer. 2023. “Downloadable Archived Fact Sheets for Healthcare Providers, Recipients and Caregivers for Pfizer-BioNTech COVID-19 Vaccine (through Summer 2023).” fda.gov. https://www.fda.gov/media/167193/download?attachment.
2022. “Physicians for Informed Consent Education: COVID-19 Vaccines.” Physicians for Informed Consent. https://physiciansforinformedconsent.org/covid-19-vaccines/.
As for removing the recommendation for pregnant women, has anyone at the DOH been paying attention to the May 21 Ron Johnson hearings when OB-GYN Dr. James Thorp provided testimony on the dangers of the COVID-19 shots during pregnancy? The Vigilant Fox wrote the following about this testimony:
OB-GYN Dr. James Thorp delivered one of the most haunting moments of the hearing.
He said the COVID shots “MIRRORED” the effects of chemical abortion drugs—and the government knew what it was doing.
Dr. Thorp pointed to the now-infamous Shimabukuro study published in the New England Journal of Medicine, which claimed a 12.6% miscarriage rate following COVID vaccination.
But when you isolate the data for women vaccinated in the first trimester, the miscarriage rate rises to 82%, Dr. Thorp said. This 82% claim remains a topic of debate within the scientific community.
If true, “This figure mirrors the effects of chemical abort drugs,” Dr. Thorp lamented.
He added, “Recently, animal studies revealed the mRNA COVID vaccine causes the destruction of 60 PERCENT of the ovarian reserve in rats.”

If that effect translates to humans, it could be a catastrophic blow to fertility and the future of entire generations.
Dr. Thorp said pregnant women were deliberately targeted, and their unborn children paid the price.
“This must stop now,” he said.
And how can the DOH be so ignorant that they never took the time to look over the Pfizer COVID-19 shot documents submitted to the FDA? In her 2024 book, Facing the Beast, Naomi Wolf reported the following:
The Volunteers found that while pregnant women were excluded from the internal studies, and thus from the EUA on which basis all pregnant women were assured the vaccine was “safe and effective,” nonetheless about 270 women were reported as pregnant in Pfizer’s post-marketing report. More than 230 of them were lost somehow to history. But of the 32 pregnant women whose outcomes were followed—28 lost their babies.
That is more than 80 percent.
The Volunteers found that a baby died after nursing from a vaccinated lactating mother and was found to have had an inflamed liver. Many babies nursing from vaccinated mothers showed agitation, gastrointestinal distress, failure to thrive (to grow), and were inconsolable.
I have heard anecdotal reports of these symptoms in babies nursing from vaccinated mothers, now, from across the country. The Pfizer documents also show that some vaccinated mothers had suppressed lactation or could produce no milk at all.
Doctors, of course, were stumped by all this. Stumped.
The National Institutes of Health (NIH) database has a preprint study making the case that there is PEG in the breast milk of vaccinated women.[footnote #10]
But what does it mean that a petroleum product is appearing in mother’s milk, when you are a tiny newborn, just arriving in the world? The NIH preprint itself reported higher levels of GI distress and sleeplessness in the infants studied, and one mother had elevated PEG levels in breast milk.
And why has the DOH never acknowledged the 173 stillbirths following the COVID-19 jab?
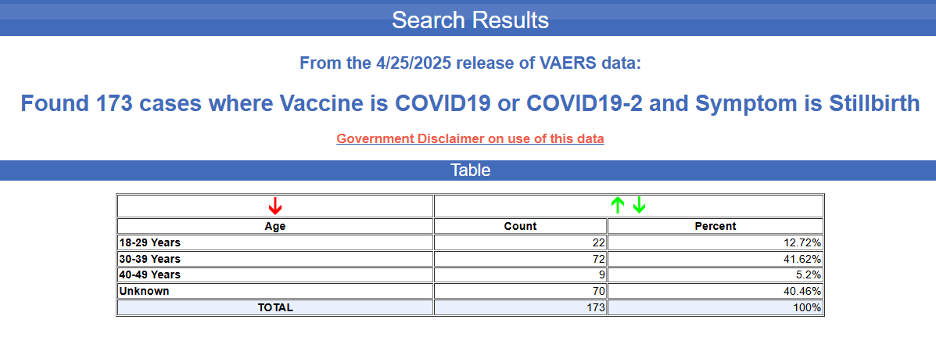
Three stillborn cases reported to VAERS occurred in Washington, as we reported on November 15, 2022.
VAERS ID: 1479059
A 31-year old’s onset began two days after taking the first dose of the Pfizer shot on May 28, 2021. Below is the submitted write-up to VAERS:
I was pregnant with a baby boy, and the due date was 09/14/2021. I took my first vaccine of Pfizer-Biontech (Lot: EW0175) on 05/28/2021. On 05/30, I started feeling short of breath and soreness on both upper arms on the afternoon. The shortness of breath lasted several hours and ended before I went to bed on 05/30. The soreness on arms lasted more than twelve hours till the afternoon of 05/31. I did no [sic] take any medicine. No other obvious reaction after the night of 05/31/2021. However, I started to feel fewer activities of the baby fewer than five days after the vaccination. On 06/08, I went to hospital and took an ultrasound to check the status of baby for the concern of no feeling of baby movement. The examine results were read by my OB doctor as everything normal of the baby with normal-high amount of amniotic fluid that makes mom feel less movement. We did see the baby move. But he was less active than what we saw on ultrasound before (20-week gestation). Another thing noticeable is that the baby did not practice breathing during the 45-minute ultrasound. The OB read it as normal to not see it so frequently on 26-week gestation. On the evening of 06/11, I went to have an emergency care as I still could not feel the baby’s movement. The doctors confirmed that my baby boy’s heart stopped beating, and the death time was within two to three days. During 06/15-06/17, I was hospitalized to do labor induction of the baby. I took oral misoprostol for inducing the labor (three times, two pills the first time, three pills the second and third time). I took both Tylenol and Ibuprofen for the fever caused by misoprostol. I took epidural around 1pm of 06/16 for anesthesia. The baby came out around 5pm of 06/16 and identified as stillbirth. On 07/16, I took my second doze of Pfizer-Biontech vaccine (Lot: EW0191) . I am in observation of my reactions.
VAERS ID: 1814238
A 34-year-old’s onset began 197 days after taking a second Pfizer dose on April 1, 2021. Below is the write-up submitted to VAERS:
Baby born stillborn to vaccinated mother. Was pregnant at start of second trimester when vaccine was received. Pregnancy seemed to progress uncomplicated. Due date was 10/8/21. Baby was moving around as had a heartbeat on 10/8/21. A scheduled C-section was set for 10/15/21. Upon arrival to hospital for scheduled C-section, the baby was found to have no heartbeat and was born stillborn. Nothing visibly wrong with baby girl (e.g. no cord wrapped around neck, no obvious trauma or deformities not viable to life, etc.).
VAERS ID: 1914564
A 28-year-old’s onset began twenty-three days after taking a second Pfizer dose on May 5, 2021. Below is the write-up submitted to VAERS:
Pregnancy 1- Chemical Pregnancy (5-week) - Miscarriage Pregnancy 2- Congenital disorder (Edwards Syndrome) - Stillbirth at 20-weeks
In his review of women’s having COVID-19 infection during pregnancy, Nicolas Hulscher’s June 14 post on The Focal Points looked at a 2021 study (Pineles et al, 2021) that found no elevated in-hospital mortality risk for pregnant women with COVID-19 compared to nonpregnant women—after controlling for symptomatic infection and comorbidities.
In fact, pregnant patients were younger, had fewer underlying conditions, and experienced significantly lower mortality rates, even among those requiring ICU care or mechanical ventilation:
In-hospital death occurred in 0.8% (n = 9) of pregnant patients and 3.5% (n = 340) of nonpregnant patients hospitalized with COVID-19 and viral pneumonia.
Among the subgroup of patients admitted to an intensive care unit, in-hospital mortality was 3.5% (9 of 255) in pregnant patients and 14.9% (283 of 1898) in nonpregnant patients.
Among those who received mechanical ventilation, in-hospital death occurred in 8.6% (9 of 105) of pregnant patients and 31.4% (294 of 937) of nonpregnant patients.
It’s important to note, as The Hill reminds readers, the “Shared clinical decision-making” section on the CDC website has the following explanation, where those who still want the shots can get them:
The CDC says children with no underlying health condition “may receive” COVID-19 vaccines, instead of broadly recommending that all children should get the inoculation. It now advises “shared clinical decision-making” between parents and physicians.
“Where the parent presents with a desire for their child to be vaccinated, children 6 months and older may receive COVID-19 vaccination, informed by the clinical judgment of a healthcare provider and personal preference and circumstances,” the guidelines now say.
The CDC website has been reporting for some time about what ‘shared clinical decision-making’ meant, as headlined in this screenshot. Of course, you have to expand the section of the website to read the full explanation.

The key phrase of the explanation: “Shared clinical decision-making vaccinations are individually based and informed by a decision process between the health care provider and the patient or parent/guardian.”
So this means that the COVID-19 shot decisions may very well be made during doctor’s visits, and this is where the DOH’s Power of Providers Initiative (POP) comes into play.
The POP began as an initiative on July 16, 2021, in response to waning demand for the COVID-19 shots in Washington.
“We are calling on all licensed healthcare professionals to talk to their patients about COVID-19 vaccines. It’s one person at a time. One conversation at a time. One vaccination at a time. It’s opportunities we should not miss at the diabetes check, at the blood pressure check, at the knee repair,” said Greg Endler, Washington State DOH Deputy Director of Health Promotion and Education.
Within a year, the Power of Providers Initiative grew to over 71,000 healthcare workers across Washington State, an excessive reach for a public health messaging effort.
The DOH “About the Power of Providers (POP) Initiative” website currently states, “POP efforts have contributed to our state having one of the highest vaccination rates in the country. With more work to do, we look forward to having you join our initiative!”
And so last Friday, the DOH sent out a letter to those providers (similar messaging appears on the POP Initiative webpage), starting with the following:
“Dear Valued Health Care Partners,
The Washington State Department of Health (DOH) is monitoring updates on federal COVID-19 vaccine recommendations and assessing how changes may impact the health and safety of Washington residents. At this time, we are not making any changes to our programs or recommendations. DOH continues to recommend that everyone 6 months and older, including pregnant people, receive the current COVID-19 vaccine to protect against severe illness.” The DOH put the last sentence in boldface; we added emphasis on the second sentence.
The POP letter then instilled its “Valued Health Care Partners” with some fear porn:
“The COVID-19 virus continues to pose serious health risks in Washington, including hospitalizations, long COVID, and preventable deaths. These risks are most prominent in pregnant people, young children, older adults, people with chronic conditions, and those who remain unvaccinated. COVID-19 vaccines remain one of our most effective tools for preventing severe illness.”
Notice in the last sentence that the DOH did not mention any of the other “effective tools for preventing severe illness,” such as hydroxychloroquine in the early stages, ivermectin, or as well as gargling and nasal flushing. Please check out our Healthy Immunity Now website and the EFU Challenge, where we’ve posted several ‘alternative’ treatment recommendations from many other licensed health providers.
The essence of the POP initiative was for healthcare providers to be aware of strategies needed to get their “most reluctant” patients to take the COVID-19 shots. At the time of the initiative launch, the DOH said, “Providers have power to fight COVID-19 with support from DOH resources that educate patients and clients on the safety and effectiveness of COVID-19 vaccines.”
The most controversial of these strategies are the tactics providers use for convincing their hesitant patients to take the COVID-19 shots:

For example, the “presumptive approach” has shown to be more effective than “participatory approach.” The presumptive approach is the attitude for the healthcare provider to presume the patient or parent is going to go along with getting the vaccine, whereas the participatory approach is to distinctly ask whether the patient wants the vaccine.
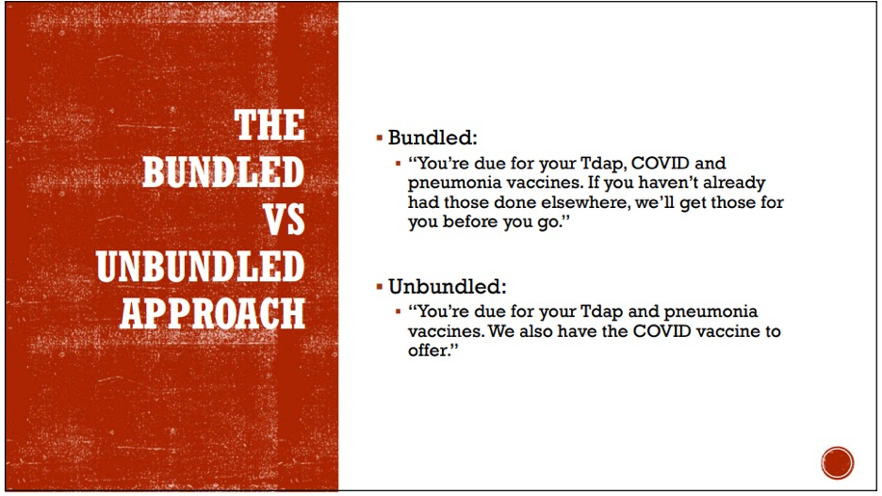
Another strategy is to go with the “bundled” as opposed to the “unbundled” approach. In other words, it’s best to suggest to the patient or parent that, besides the shots that are “due,” the COVID-19 shot is also available.
As for the discussion strategy in itself for those patients reluctant to take the COVID-19 shot, the following “3A” approach is executed:

Healthcare providers are also instructed to tell their patients that they, themselves, and their family members have taken the COVID-19 shots.

POP participants are also instructed to educate their patients in two futuristic areas. First, more COVID-19 boosters are likely forthcoming, and this shows that the COVID-19 shots have become part of the regular schedule (as ICWA members predicted), so it’s best to get one now. Second, the COVID-19 shots protect people from severe illness and even from other things that we may not know about yet.
ICWA members saw this seasonal recommendation coming long ago, knowing that manufacturers and sock-puppet agency approval authorities were angling for the liability shield provided by the National Childhood Vaccine Injury Program (the 1986 Act). Many members successfully warned the public in November of 2020 with 100-foot-wide banners displayed over many Washington freeway overpasses as they participated in Joshua Coleman’s V is for Vaccine worldwide demonstration.

Department of Health Punishes Long-Term Care Facilities with Rewards
In his book Punished by Rewards, Alfie Kohn writes in the chapter “Skinner-Boxed” about how rewards stymie critical thinking and creativity.
In that chapter, he writes the following about this do-as-you’re-told mentality:
Teresa Amabile, who specializes in this topic, asks us to picture a rat in the behaviorist’s maze trying to find its way to the cheese. The rat does not stop to weigh the advantages of trying another route, starting off on a path where the cheddar smell is less pronounced in the hope of finding a clever shortcut. No, it just runs toward where it thinks its breakfast waits, as fast as its tiny legs can take it. “The safest, surest, and fastest way out of the maze [is] the well-worn pathway, the uncreative route,” says Amabile. “The more single-mindedly an external goal is pursued, the less likely . . . that creative possibilities will be explored.” The narrow focus induced by rewards is similarly worrisome, she adds, since being open to “the seemingly irrelevant aspects [of a task] might be precisely what is required for creativity.”
This leads us to wonder if the Washington Department of Health thinks of long-term care workers—and volunteers—as mice for its Long-Term Care Respiratory Immunization Awards program:
The program recognizes LTC facilities, nursing homes, and agencies in Washington that meet or exceed vaccine award threshold rates among their staff. This staff vaccination award recognition program launched in 2021 during the COVID-19 pandemic. Now it is an annual LTC staff vaccination award. Annual award enrollment and data submission begins in February and runs through May. Award packets are targeted for delivery in October. . . . For 2024-2025, minimum staff vaccination rates to qualify for an award are 40% flu AND 20% COVID-19.
So instead of encouraging LTC facilities to weigh the pros and cons of vaccinating their employees, the DOH is offering rewards as a marketing tool get to more healthcare workers vaccinated.

And instead of a fresh slice of highly aromatic cheddar cheese, here’s what a winning facility gets:
If your facility met one of the award thresholds, registered to participate, and submitted site data, keep an eye out for your Awardee Recognition Packet, which will arrive via USPS mail this fall.
Each packet includes:
A site award door/window cling for on-site display
An electronic award logo for use on websites or print materials
A signed recognition letter from the Secretary of Health
A frameable certificate signed by the Governor
Thank you for your continued efforts to reduce vaccine-preventable respiratory diseases in long-term care settings.
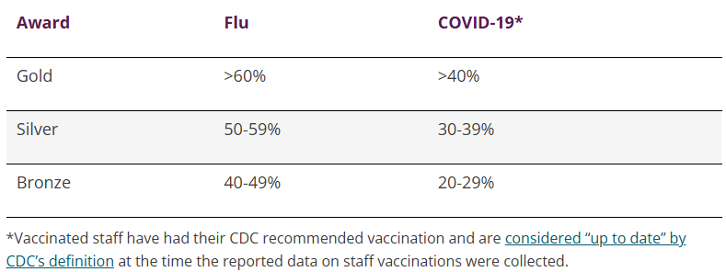
The table below shows the percentage of healthcare worker vaccination rates and the corresponding award levels. For 2024-2025, minimum staff vaccination rates to qualify for an award are 40% flu AND 20% COVID-19. For example, to achieve the Silver Award, you would need 50% for flu and 30% for COVID-19. In another example, if you achieved 59% for flu and 39% for COVID-19, that would also result in the Silver Award. If you achieved 49% for flu and 35% for COVID-19, the result would be a Bronze award.
To qualify for the Long-Term Care Respiratory Immunization Award, facilities were required to do the following:
Know one vaccination barrier for paid employees and volunteers at the LTC location.
Fill out the registration survey between February 3 and May 31, 2025.
Determine the highest percentage of vaccinated employees working in the facility from May 1, 2024 to April 30, 2025.
Fill out the final survey to report data by June 2, 2025.
ICWA and CHD Members to March in Covington Days Parade
You can join Informed Choice Washington and the Washington chapter of Children's Health Defense in the Covington Days Parade on Saturday, July 19! The effort, led by ICWA’s South Puget Sound team, will meet at 9:00 AM for a 10:00 AM start. They anticipate to be done marching by 11:00 or 11:30 AM. This isn’t just a parade—it’s an energizing, high-visibility opportunity to engage hundreds of new people with our message of informed medical choice. With a MAHA tailwind, you can help carry a banner, hand out flyers and ‘healthy’ candy, or just walk with other members of the health freedom movement. The first 30 participants to sign up and show up will receive a cool CHD branded tote or glass water bottle.

Just send an email to lisa@informedchoicewa.org if you are interested or have questions.