

ICWA Weekly News 11-1-23
ICWA Weekly News 11-1-23
DOH reminds everyone to use VAERS - but says nothing about the data already there; Silent Majority Foundation represents Dr. Michael Turner in two key lawsuits; Upcoming Events; Radio Show links

In this Issue:
DOH Webinar Falls Short on VAERS
Silent Majority Foundation Represents Dr. Turner in Two Cases that shouldn’t have ever been needed, but he practices in Washington State
Upcoming Events: Be Brave Washington meets tonight in Lyndon.
Radio Show Links
DOH Webinar Falls Short on VAERS
The COVID-19 Vaccine and RSV Vaccine Updates Webinar last October 24th had a surprising moment when Heidi Kelly from the Washington Department of Health (DOH) ended her presentation by reminding providers of the importance of the Vaccine Adverse Event Reporting System – or VAERS:

Kelly initially thought she was done with her presentation, but then caught herself:
I believe that’s all I have…also, whoops…um…very important piece. If you or someone you know or a patient does experience a vaccine adverse event, please make sure that you report it. It helps with the nation’s early warning system for vaccine safety. It’s one of the many aspects of data collection that they do. So, and as you know, when we were doing J & J (Johnson & Johnson), it was a good example. They were pulling information off VAERS and other systems to figure out that there might be an issue. They pulled it out. They relooked how they were going to offer it, and then eventually pulled it off the market. So it is really important, they do use this data to ensure that everything is still safe and rolling.
Kelly made a valid point about this need, especially considering the underreporting of deaths from the COVID-19 shots here in Washington. For example, when Jay Bonnar provided Steve Kirsch with a rundown of fifteen people he knew in the Seattle area who died suddenly after taking the COVID-19 shot, only the death of Jessica Berg Wilson (VAERS ID: 1683324) has been reported to VAERS. (See ICWA Weekly News from August 28th, Webinar Slides, Webinar Video)
But if this is such an “important piece,” why doesn’t the DOH supply the VAERS data to accompany all the other statistics, graphs, and reports on its website?
For example, the DOH never shows, much less mentions at this webinar, the following adverse events after taking the COVID-19 shots reported to VAERS here in Washington:
222 deaths
135 cases of myocarditis
115 cases of pulmonary embolism in which six resulted in death
17 cases of Ischaemic Stroke
As for J & J and its subsidiary Janssen, Kelly was referring to the blood clotting issues, which were detailed in a May 6, 2022 issue of The Defender. “The FDA said it has identified sixty cases of vaccine-induced thrombosis with thrombocytopenia syndrome, including nine deaths, out of about 18 million doses administered — although the condition is likely underreported.”
VAERS lists 2,821 deaths after taking the Janssen shots:

But with 2,821 deaths being reported from the Janssen shots, one is left one wondering why the Pfizer/Biontech shots have not been pulled after 22,197 deaths (121 here in Washington) have been reported to VAERS or why the Moderna shots have not been pulled after 10,531 deaths have been reported to VAERS.
As much as Kelly can be commended for breaking away from the DOH tradition of avoiding discussion of VAERS, she still promoted the DOH’s consistent message that it’s OK to mix the COVID-19 shots with RSV and flu shots without providing any supporting safety or efficacy data. We covered this quickly last week, and go into more detail here.
She showed the five hundred nurses and medical assistants attending the webinar slide 10:

There was hope that the above link to the Health Alert Network (HAN), intended for quick communications to healthcare workers, would finally provide the clinical data to support the efficacy and safety of combining these shots.
Yet, we weren’t surprised that the only mention of the co-administration topic on this site fails to reference any studies – just the judgement call of the doctor, along with what they called ‘patient preferences.’
Healthcare providers can co-administer the vaccines for which a patient is eligible in the same visit, including RSV, COVID-19, and influenza vaccines. When deciding whether to co-administer other vaccines with RSV vaccine at the same visit, providers can consider whether the patient is up to date with currently recommended vaccines, the feasibility of their returning for additional vaccine doses, their risk of acquiring vaccine-preventable disease, the vaccine reactogenicity profiles, and patient preferences.
Francis Bell, MD, representing Swedish Pediatric Infectious Diseases, said the following about mixing the RSV shots designed for those sixty and over with COVID-19 shots:
Co-administration with other vaccines that might be due, in particular flu and COVID, is considered acceptable. This should be discussed with your patient. Some patients will want them one at a time, and that’s totally fine. But if we are worried that the patient may not come back, then this is the time to seize the opportunity, for it’s okay to give all three together.
Bell spoke highly of the Morbidity and Mortality Weekly Reports (MMWR) as his source and referred the webinar’s participants to the following link:
But this one MMWR article only states that “evidence is mixed” and “Data are lacking on the safety” for mixing shots in older adults:
Administering RSV vaccine with one or more other vaccines at the same visit might increase local or systemic reactogenicity. Data are only available for coadministration of RSV and influenza vaccines, and evidence is mixed regarding increased reactogenicity. Data are lacking on the safety of coadministration with other vaccines that might be recommended for persons in this age group, such as COVID-19 vaccines; pneumococcal vaccines; adult tetanus, diphtheria, and pertussis vaccines; and the recombinant zoster vaccine (the recombinant zoster vaccine and GSK’s RSV vaccine contains the same adjuvant).
Dr. Bell had plenty of time to promote the new RSV products from Glaxo-Smith-Kline (RSVPreF3 recombinant protein, aka Arexvy) and Pfizer (RSVPreF recombinant protein, aka: Abrysvo), but didn’t have time to gather any re-assuring information on co-administration of shots or to warn of danger signals from the RSV shots that were just put on the market.
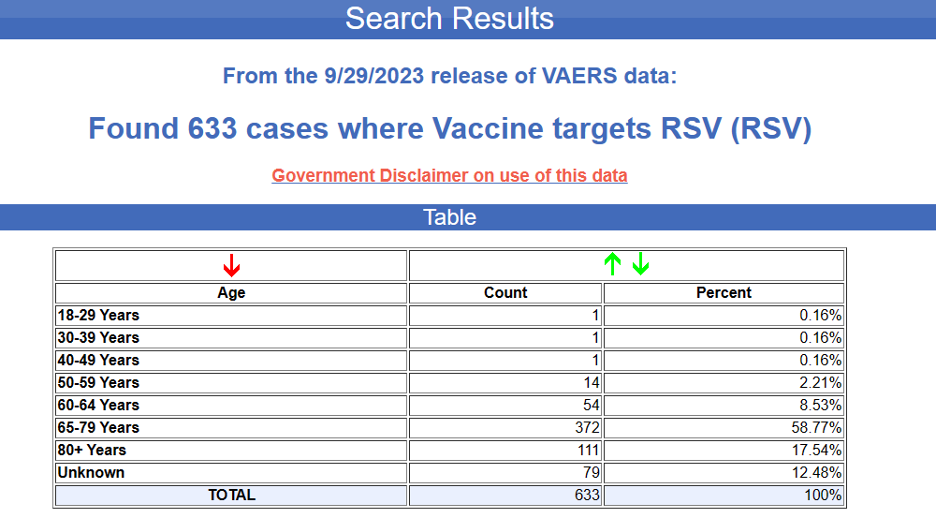
During the question and answer period, Dr. Bell said that the only side effect of the RSV shots was an occasional redness in the arm. Yet, VAERS shows of the 633 reports from the Arexvy RSV shot since the CDC recommended it last June, where two resulted in death.
The first death was of a 102-year-old female, entered on September 19 of this year.
VAERS ID: 2683686
She had chills and felt achy the same evening after taking the shot earlier in the day on September 12, 2023 . She died two days later.
The second was of a 71-year-old in California, entered on September 21 of this year.
VAERS ID: 2684944
He received the vaccinations on September 5, 2023. He then had increased coughing and a fever in less than twenty-four hours. These symptoms lasted for four days after the vaccine, which is when he was found deceased at home.
VAERS lists nineteen cases in Washington of adverse events following the RSV shots.

The following examples show that the side effects can be much more than the red arm that Dr. Bell had described during the webinar. Readers should note that these reports have been submitted over only a few months since the shots became available. (Notable comments have been bolded).
75-year-old female, VAERS ID: 2675112
Submitted write-up; Severe sleepiness to the point of sleep paralysis continuing for about 24 hours from onset at 10 hours after vaccine. Nausea, diarrhea, dizziness, lack of appetite, headache, swollen Left arm (size of grapefruit, hot hard, itchy, red) from hour 10 thru bedtime on day 2. Swollen arm symptoms and diarrhea continuing thru day 3 and 4.
66-year-old female, VAERS ID: 2681657
Submitted write-up: About 10 hours after shot I started having the chills. I spiked a fever and developed body aches and shaking . I developed a headache and nasal congestion. Followed by nausea and felt delusional. I took an advil at 1:30 am and my symptoms subsided and I was able to go to sleep. I took another Advil in the morning I think around 7 . As of this writing @ 2 pm, I have low grade body aches , headache and feel like I have a cold. I will take another Advil in an hour or two and expect to feel better by tomorrow.
72-year-old female, VAERS ID: 2682121
Submitted write-up: 08-SEP-2023 Reporter was the patient, who accidently received 2 doses of Arexvy on Wednesday. The patient experienced diarrhea on Thursday morning which resolved midday. She experienced body aches late Thursday for which she took Tylenol and resolved when she woke up today (on the day of reporting). The patient received accidentally received 2 dose Arexvy on same day, which led accidental overdose.
65-year-old female, VAERS ID: 2682609
Submitted write-up: Patient describes tingling, high fever (103 degrees) and fatigue
76-year-old female, VAERS ID: 2682766
Submitted write-up: Vaccine administered in retail environment so above manufacturer information is not accurate. Hours after receiving RSV and flu vaccine together she experienced an acute confusional episode. Went to ER and had negative workup after which her mentation cleared.
69-year-old female, VAERS ID: 2682871
Submitted write-up: Headache, redness and itchiness at injection site, nausea; patient says side effects started immediately and lasted for 1 week.
82-year-old male, VAERS ID: 2685609
Submitted write-up: RSV GIVEN WITH THE HIGH DOSE FLU VACCINE 22 hours later fever, nausea and one episode of vomiting, anorexia
73-year-old female, VAERS ID: 2686227
Submitted write-up: Approximately eleven hours after vaccination patient reports extreme chills, increased blood pressure, irregular heart rate, and headache. This reaction prompted a call to EMS. Emergency responders medically evaluated the patient and confirmed hypertensive status and irregular heartbeat suggesting patient follow up with her cardiologist. Patient is now recovered.
From these example reports, submitted over only a few months, it seems that Dr. Bell is not reviewing the VAERS database or not telling people the full story.
Silent Majority Foundation Represents Dr. Turner in Two Cases
On an October 21st Saturday morning, Pete Serrano stood above his audience at the Great Northwest Awakening in the Clark County Events Center and said, “You are the reason that this fight has to continue.”
He explained that the Silent Majority Foundation (SMF) was birthed out of necessity as the people have watched the ruination of our Constitutional Republic. “The Constitution is what stands between the government, you, and God and ensures that the government is held in check.”
After he talked about one of his multiple cases where Governor Jay Inslee is named as a defendant, and his case that was filed that apparently caused the school mask mandates to be dropped, he delved into his court battles with the Washington Medical Commission. “We see the way these doctors are being persecuted is changing day-by-day,” he said.
Video of Pete Serrano esq. at the Great Northwest Awakening [14 mins]
Then the SMF wrote to its supporters last Wednesday that, “It’s our pleasure to stand with courageous doctors who are willing to buck the system to save lives.” In particular, Dr. Michael Turner is plaintiff in two cases filed with the SMF.
Dr. Turner has a very impressive resume: He’s a graduate of Stanford University, Harvard Medical School, and has worked for the Mayo Clinic. He is an Integrative Medicine physician and CEO of his own concierge practice, mainly serving Richland and the Tri-Cities area.
He is the lead plaintiff challenging the Washington Medical Commission’s COVID-19 Misinformation Position Statement in an attempt to protect the free speech of Doctors across Washington and to hold the Washington Medical Commission accountable for using a Position Statement, disguised as a lawful rule, to punish doctors.
After the SMF sued the Washington Medical Commission, they asked the judge to enjoin the enforcement of the unlawful position statement for two reasons:
It was passed without allowing doctors or the public to comment on it (among other omissions) -- a violation of the Administrative Procedures Act, and
It violated doctors' free speech by punishing them for talking about COVID -19 treatments the Commission disapproved of.
The judge refused to rule on our preliminary injunction. Instead, he chose to stay it until all the doctors had their hearings in front of the Washington Medical Commission.
The SMF asked for reconsideration, but the judge refused to reconsider his ruling. “Therefore, we are considering filing a motion for discretionary review with the appeals court,” SMF says. “Recently, Dr. Eggleston has been granted discretionary review on similar grounds we are claiming in this case.”
Dr. Turner is also facing a challenge against his license. He helped many patients during the pandemic by prescribing ivermectin among other early nutraceuticals to attempt to help reduce their chances of landing in the hospital. For this, he is being brought in front of the Washington Medical Commission on charges that he has committed unprofessional conduct. Silent Majority Foundation is defending him in this challenge.

The case synopsis below is in Dr. Turner's words. It addresses his experience with the Washington Medical Commission and how the Commission has attempted to regulate his practice.
In case you missed it, I am listed as the chief plaintiff in a little piece of jurisprudence called Turner et al. vs. Washington Medical Commission lawsuit (accompanied by fellow intrepid doctors like Dr. Renata Moon, Dr. Ryan Cole and Dr. Richard Wilkinson).
This garnered a bunch of press – everything from front-page billing on the Sunday edition of our local paper, to RFK Jr’s Children’s Health Defense, and even an editorial in the British Medical Journal (God save the Queen!). We had our first hearing last week and I have to say that our attorney -- Pete Serrano Esq.– did an absolutely superlative job. (Thank you Pete, and all of your talented and dedicated team at the Silent Majority Foundation. It is time to be silent no longer.)
On the surface, the issue revolves around providing Ivermectin (and other early treatments) as a telemedicine option.
As you know, Ivermectin and Hydroxychloroquine were stigmatized by the media, mainstream medical organizations, federal health institutions and state medical boards. The WA state medical commission (WMC) published a “COVID 10 misinformation statement” that cited the FDA as establishing the “standard of care”, and then boldly warned practitioners to “take note” that Ivermectin and Hydroxychloroquine are not FDA-approved for COVID.
Then -- just to make it convenient to squash such terrible care -- they conveniently provide a link to file a complaint and “encourage” the public and other practitioners to report any deviation from this standard of care.
Of course, I find this absurd and abusive on many levels:
1) The FDA does not have the mandate, authority nor expertise to determine what specific medicine may or may not benefit a particular patient at a particular point in time.
2) “Off-label” medication usage is common and appropriate in the right context
3) Complaints were accepted and used as a basis for investigation that were not even filed by the patient nor his/her immediate family.
I repeat: none of these complaints ever came from my patients or even close family members.
(On the contrary, my early treatment patients and family have overwhelmingly expressed appreciation and gratitude.)
One complaint, for example, came from an ER doctor after looking over my patient’s medication list. Another came from the patient’s granddaughter who lived across the state and was upset when she heard that grandma was given Ivermectin (I am not making this up).
Furthermore, none of my patients suffered any harm that could be directly tied to my treatments. In fact, looking back, my use of these medications was resoundingly successful, and I continue to be astounded with stories of hospitalizations averted and lives saved.
We, as plaintiffs, believe that these investigations into our licenses are an attempt to punish us for violating this “position statement” – a statement, which, contrary to due political process, is being treated and enforced as a “rule”, when it in fact has no such legal standing.
The SMF says this case comes down to First Amendment rights:
The First Amendment states, “Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the right of the people peaceably to assemble, and to petition the Government for a redress of grievances.” If our physicians are no longer “allowed” to freely advise their patients or make public statements that are outside of a prescribed narrative then we do not have medical freedom, we have tyranny.”
More details about these two cases and other Silent Majority Foundation efforts can be found at these two links:
Home - Silent Majority Foundation
Silent Majority Foundation (locals.com)
November Washington Events
Be Brave Washington will meet tonight, Wednesday, November 1st at 7 p.m. at the VFW Post 9301 at 7011 Hannegan Road in Lynden. Social/Networking time begins at 6 p.m.
The Washington Board of Health (BOH) will meet on Wednesday, November 8, from 9:30 a.m. to 2:50 p.m. The meeting will be in Tumwater at 111 Israel Road SE in rooms 166 and 167 in the Building Town Center. Instead of Keith Grellner, Patty Hayes will be serving as chair. Draft Agenda
Public Comments begin at 9:50. The board encourages those wishing to make public comment to sign up with the board at wsboh@sboh.wa.gov. For those wishing to give public comment through Zoom, sign up through the Zoom webinar link by 12:00 Noon the last business day before the meeting. Your name will be called when it’s your turn to comment.
To access the meeting online and to register: https://us02web.zoom.us/webinar/register/WN_LWdVVDUbTgi7WPrgEOx3BQ
Written comments are best if sent in by Friday at noon to wsboh@sboh.wa.gov.
Of special note, at 1 p.m. the board has allotted one-and-a-half hours for a “Climate Change Story Telling Panel.”
Medical Freedom Forum: Be Informed, Be Unafraid
November 11th, Deer Park (Spokane), 10 AM to 3 PM.
A free event. REGISTER HERE

Seattle Truth Network Event
Connect in Person
Thursday November 16th from 6:00 to 9:00 PM at Razzi's Pizzeria in Greenwood in the Party Room downstairs
8523 Greenwood Ave N, Seattle
Dinner and conversation starts at 6:00; Meeting at 7:00
Catching up on current events PLUS a Topic to be announced.
October 27 Episode of An Informed Life Radio - show links
Jodi O’Malley, nurse whistleblower and hospital insider, as well as compounding pharmacist Shawn Needham appear on ‘An Informed Life Radio’ this week. Viewers learn both Jodi and Shawn’s perspectives on the current system of healthcare and how it is being transformed.
Hour 1
Hour 2