
ICWA Weekly News 7-3-24
SCOTUS decisions to check growth of Deep State; POTS adverse events in WA; Two WA docs claim COVID shots reduce risk of myocarditis; Protocol 7 movie on July 10-11, Voter Guide; The Guano Report


In this issue:
Two Supreme Court Decisions Expected to Check Growth of Administrative State
POTS Adverse Events in Washington following COVID-19 Shots
Debunking Two Seattle Doctors Claims that “Unvaccinated” are More at Risk of Myocarditis
Upcoming Events:
July 10,11: Protocol 7 in Seattle & Spokane Valley; as well as Tigard & Salem (OR)
September: Vaxxed III – The People’s Study premieres through Gathr.com
Just Released: WA Voter Guide from Stand for Health Freedom
The Guano Report: a weekly reminder to say EFU to the Bird Flu
June 28 Episode of Informed Life Radio - - Notes and links
Health hour: Molds & Mycotoxins
Guest: Melissa Schreibfeder BSN, RN
Founder of the Functional Nurse Academy discusses the health issues caused by exposure to mold and mycotoxins and treatment options from a functional medicine perspective.
More about GMP certification for supplements (General best-practice Manufacturing Practices)
https://www.americaoutloud.news/category/podcasts/nurses-out-loud/
Liberty Hour: Health Freedom News
CDC ACIP Meeting June 26 - Age Raised to 75 years old for RSV
Quick Quotes: The ACIP chair, Dr. Helen Talbot, said some providers aren’t recommending the COVID-19 vaccines because they’re concerned for their own safety when recommending the vaccine to people who did not want it.
“There has been increasing physical and verbal abuse in hospitals and outpatient healthcare settings,” she said. “This is a very sensitive topic to many people and some of our physicians may not be recommending it due to concerns about safety for them and their staff.” “I think that is something that needs to be quantified and studied,” she said. [ICWA has many questions on this and wonder what this could be setting up].
Dr. Camille Kotton said it will be difficult to “flip” the 40-50% of Americans who have now said they will never get a COVID-19 vaccine. [read: any vaccine?]
Defender reported on MedPage Today press release: WA State Doctor Lin Fined (May 12) for prescribing ivermectin (a whole 5 instances).
Employees v. United granted nationwide class-action status in Texas may cost airline nearly $1B for religious discrimination. (Washington Examiner June 27)
Sign up to hear about the methods used against your kids on sports teams:
Supreme Court social media posts decision is a win for Biden (usatoday.com) [Cognitive Dissonance Alert: Why would USA Today celebrate U.S. Government censorship? Aren’t they a media company?]
Doctors Protecting Children petition
At least five recent court decisions re-affirm religious exemptions for medical mandates, and could help appeal New Yorkers for Religious Liberty v. The City of New York Case No. 22-1801.
1. Does 1-11 v. Board of Regents of University of Colorado, 100 F.4th 1251 (10th Cir. 2024)
2. Health Freedom Def. Fund, Inc., v. Carvalho, No. 22-55908, 2024 WL 2873372 (9th Cir. June 7, 2024)
3. Bacon v. Woodward, No. 22-35611, 2024 WL 3034850 (9th Cir. June 18, 2024)
4. Lucky v. Landmark Med. of Michigan, P.C., No. 23-2030, 2024 WL 2947920 (6th Cir. June 12, 2024)
5. Ringhofer v. Mayo Clinic Ambulance, 102 F.4th 894 (8th Cir. 2024)
Two Supreme Court Decisions Expected to Check Growth of Administrative State
As disappointing as last week’s Supreme Court’s 6-3 ruling was when it favored President Biden in the Murthy versus Missouri censorship case on grounds of muddled “standing” (so many entities were censoring, the Court said it couldn’t tell for sure what role the government played), the People did receive two pieces of good news during that same week’s series of rulings. Two Supreme Court decisions went against the administrative state, often referred to as the deep state. There is a chance that these cases could have a bearing on the Ninth Circuit Court of Appeals in the Stockton versus Ferguson case.
Back on May 22, In the United States District Court, Eastern District of Washington, Judge Thomas O. Rice dismissed the First Amendment free speech case pursued by Children’s Health Defense (CHD) lawyers, including Robert F. Kennedy Jr., against Attorney General Bob Ferguson and the Washington Medical Commission (WMC) for silencing doctors’ public speech. Stockton v Ferguson plaintiffs included NBA legend John Stockton of Spokane, Dr. Richard Eggleston, Dr. Thomas Siler, Dr. Dan Moynihan, members of the Washington chapter of Children’s Health Defense, and many as-yet unnamed plaintiffs who have all experienced the effects of ill-founded WMC policies.
Rick Jaffe, lead counsel for CHD on this case, is appealing to the Ninth Circuit. We can speculate that the appeal may benefit from two of the new Supreme Court rulings, even though CHD’s main complaint aims to protect doctor’s ability to speak publicly.
The first possibly-relevant decision came last Thursday when, in a 6-3 vote in the Jarkezy case, the Supreme Court held that people accused of fraud by the SEC have a Constitutional right to a jury trial in federal court, as opposed to the in-house proceedings the SEC likes to use in civil fraud complaints. Jarkezy’s lawyers noted that the SEC wins almost all the cases it brings in front of its own administrative law judges, but it only wins around half (60%) of the cases it tries in federal court before juries.
Could this cause the WMC to conduct jury trials instead of in-house investigations that levy fines and revoke licenses? After all, the WMC is an executive branch Commission like the Securities and Exchange Commission, except at the state level. Wouldn’t that be interesting to actually hear the evidence in a doctor’s public speech case?
In his Coffee and Covid Substack on June 28, Jeff Childers wrote about this dismantling of the administrative state, borrowing words from the dissenting justice Sotomayor:
The opinion included some pretty solid quotes. Chief Justice John Roberts wrote for the majority, holding that “A defendant facing a fraud suit has the right to be tried by a jury of his peers before a neutral adjudicator.” But Justice Sonia Sotomayor, who spitefully read her dissent aloud in the courtroom, complaining that people “who seek to dismantle the administrative state” would surely ‘rejoice’ in the majority’s decision.
That includes me! Dismantle the Administrative State! Do it now! The decision isn’t limited to the SEC. It effectively cut off all Executive Branch agencies from convicting Americans without due process. Speaking of the Administrative State, closely synonymous for ‘the Deep State,’ we still await the Court’s Chevron adjustment in the Loper-Bright case. Yesterday’s decision was a terrific signal that the Administrative State may be about to meet the judicial weed-whacker.
That decision on the Chevron case came the very next day with the Supreme Court again ruling, in a 6 to 3 vote, against the ability of government agencies to interpret and make rules on their own. It wasn’t just an adjustment to the 40-year-old Chevron decision – it overturned it. Dr. Robert Malone wrote the following analysis of the decision:
In a major blow to US Federal Administrative State power, the US Supreme Court overturned the Chevron Deference precedent by a 6 to 3 vote. Chevron deference is an administrative law principle that compels federal courts to defer to a federal agency’s interpretation of an ambiguous or unclear statute that Congress delegated to the agency to administer. As a consequence, executive branch administrative agencies have been able to step into the policy and power vacuums created when the legislative branch fails to define legislative intent clearly, and to functionally define law and policy as each agency sees fit.
Today’s majority opinion states that “Chevron, decided in 1984 by a bare quorum of six Justices, triggered a marked departure from the traditional judicial approach of independently examining each statute to determine its meaning. “
The Chevron Deference principle was established in the 1984 U.S. Supreme Court case Chevron U.S.A., Inc. v. Natural Resources Defense Council, Inc. Conservatives have long argued that this precedent represents judicial activism at its worst and violates fundamental aspects of the constitutionally defined separation of powers by empowering executive branch administrative agencies to functionally make law. Liberals have argued that It allows agencies to implement laws and regulations more flexibly, giving them the authority to interpret ambiguous statutes. This way of thinking believes such delegation of authority to the bureaucracy can lead to more efficient and effective regulation, as agencies are better equipped to address complex issues than the legislature is.
Since the 1984 case, the resulting explosive growth of administrative agencies and their budgets, coupled with Chevron-associated legal barriers to administrative accountability, has given rise to a massive, arrogant, parasitic administrative state that has come to believe that its actions and motivations are above reproach or questioning. This doctrine has underpinned the arrogance of Dr. Anthony Fauci and colleagues at NIH so recently on display in congressional hearings for all who wish to see it. This case has enabled the administrative state to grow so large that many agencies have developed their own judiciary. Prosecutors and judges are unique to each agency, with the power to indict and force you to go to trial all within the structure of the agency - basically, each agency creates its own law and then acts as judge, prosecutor, and jury. No separation of powers, just one hand washing the other, all unified collusion. A self-contained, unconstitutional fourth branch of government with each agency operating under the protective legal umbrella of being defined as the ultimate authority in all matters involving legislative - or scientific and technical- interpretations.
Jeffrey Tucker, founder and president at Brownstone Institute gave the following commentary on the Chevron ruling in an article dubbed It’s Darkest Before Dawn:
Is there no hope? Of course there is. Just this morning, the day after the debate disaster and two days following the court’s terrible decision on free speech, a central pillar of administrative totalitarianism was toppled by the court. The so-called Chevron Deference is over. Finally, we have some clarity on what agencies can and cannot do at their own discretion. It’s a big win, but about 1% of what is necessary to regain rights and liberties.
Again, we speculate that Loper-Bright could have bearing on the Stockton v Ferguson case. We should recall that Stockton et al and other doctors filed against the WMC because they suddenly, and without due process, instituted a new policy that gave them cover to investigate licensed doctors who spoke out against the COVID narrative. If the WMC faced more legislative oversight of its rulemaking, it might not have been able to pass this policy, thereby having no basis to investigate doctors in the first place. It remains to be seen if these federal cases will have bearing on state-level agencies and their rule-making authority.
Besides these Supreme Court decisions, we should note that the Stockton versus Ferguson case may have received another boost when the American Physicians and Surgeons (AAPS) scored a landmark First Amendment/Free Speech victory on June 3.
In this similar case, the influential United States Court of Appeals for the Fifth Circuit held that there is a constitutional “right to hear” that enables a sponsor of conferences, such as AAPS, to challenge censorship that chills presentations at its events.
POTS Adverse Events in Washington following COVID-19 Shots
Last Wednesday, The Expose’ published an article about the United States army admitting that a Moderna COVID-19 shot had caused postural orthostatic tachycardia syndrome or POTS to a national guard specialist.
The article began with the following summary:
US Army National Guard Specialist Karoline Stancik, 24, has reportedly racked up over $70,000 in medical debt after being hospitalised for heart complications due to Moderna covid injections.
After her first dose, she developed a headache, sinus problems, cough and chest pain. After her second dose a month later, she developed intense adverse reactions, including high heart rate, dizziness, neuropathic pain and difficulty breathing. She suffered her first heart attack after receiving the second dose of Moderna’s covid “vaccine.”
Stancik has now had three heart attacks and a stroke and, at the age of 24, is having a pacemaker fitted.
An Army memo about Stancik’s situation, acquired by Investigative Journalist Catherine Herridge, showed she had been diagnosed with postural orthostatic tachycardia syndrome or POTS.
The memo from the US Department of the Army’s Human Resources Command acknowledged she was diagnosed with POTS:

And that research linked COVID-19 infection and mRNA shots, albeit ‘to a lesser degree:’

Looking at VAERS, 976 cases of POTS following the COVID-19 shot in the United States and its territories have been reported.
Supporting the case for more investigation is that onset for 103 of the 976 POTS reports occurred within twenty-four hours after taking the COVID-19 shot.
In Washington, twenty-three cases of POTS have been reported to VAERS following the COVID-19 shots.

The onset for four of those POTS events occurred within twenty-four hours after taking this shot. Below are summary write-ups of those four cases in Washington:
VAERS ID: 1446328
14-year-old male one day after a second Pfizer shot on May 14, 2021. He had no preexisting conditions. Submitted write up: Symptomatic with POTS (Postural Orthostatic Tachycardia Syndrome), chest pain, short of breath.
VAERS ID: 2083502
38-year-old female with the onset occurring one day after taking a Moderna shot on April 7, 2021. She had no preexisting conditions. Submitted write-up: Patient felt poorly for weeks after the first Covid 19 vaccine on 3/19/2021.She recovered enough for the second dose. After that she did not recover. Dysautonomia symptoms, chest pain, heart pulpitatibrain, heart rate fluctuating between lower 40s to 160s, shortness of breath and tremors after mild exertion, extreme low blood pressure, fog, swelling of legs when standing, feeling very ill, insomnia, interrupted sleeping pattern, extreme fatigue, Small muscle spasms & sudden reflex sending electric shock waves through body leaving a tingly sensation behind. For months light touch was irritating or painful as this became less of a problem joint pains started.
VAERS ID: 2101656
31-year-old female in which the onset began one day after taking the second Pfizer shot. Preexisting conditions were joint pain and acid reflux. Submitted write-up: Within a day, developed chest pain, tightness, heaviness, palpitations. Progressed over time. Repeated ER visits. Later diagnosed with Postural Orthostatic Tachycardia Syndrome. Am now completely bedridden.
VAERS ID: 2278382
32-year-old female onset began one day after taking a third Moderna shot. Only preexisting condition was “environmental allergies.” Submitted write-up: Initial symptom was chills with the development of tension headache with numbness and radiation down neck. Initially thought reaction to shellfish, ruled out. Symptoms progressed to development of chronic, debilitating POTS. She described episodes of intense fatigue, "adrenaline surges," anxiety, and tachycardia. Her resting HR is 40-60. When standing, it will spike to 110 then go down to 95-100. If she raises her left arm, her HR can go up to 130. She was home/bedbound for about 3-4 months in an attempt to keep her HR stable and had to take leave/dramatically reduce work hours. Her symptoms improved slightly with 12.5mg sertraline, vitamin supplements, and an herbal remedy, but she still has flares.
Last April, the Children’s Health Defense People’s Study documented on video a Port Townsend resident who had a POTS diagnosis after taking the COVID-19 shot.
Sol Riou was a social worker at a primary care clinic for Jefferson Healthcare. She would get referrals from doctors for attending to their patients’ emotional problems.
“One day, we were told we could not see anybody because there was a pandemic going around,” she said. “It was a nightmare of mixed information. One lady said that after she had received the COVID-19 shot she had migraines all day long. All the things that doctors normally give for migraines did not help her. The patient said that even though she had the migraines the day after the vaccine, the doctors said that it had nothing to do with the shot. The patient did not believe them.”
After Sol gave rundowns of three heart issues that occurred after the COVID-19 shots, she said that she did not want to take the jab. She said that the nurses kept coming to her office and telling her that they had extra vaccines and that this would be a good time to take the shot. There was tremendous pressure from all around to get vaccinated. There was no confidentiality with this, either. The front desk attendants were going down patient lists and calling them to make appointments to get the COVID-19 shots.
Sol explained in more detail what happened from there.
One day I woke up sick and was tested for COVID. It took three days to get the results back. I was sitting there, three days quarantined and thought that if this test comes up positive, I would be the first person in this hospital who was a staff person who got COVID and went to work with COVID. I live in a small town, so I would have been on the front page of the newspaper, and everyone knew I was unvaccinated, and so I thought that if I got COVID, I could at least say that I was vaccinated. If I knew of anyone else who had not been vaccinated, then I would feel okay about not getting vaccinated.
On Friday, I got vaccinated, and on Tuesday I woke up and said, “What’s the matter?” I couldn’t think or focus. I didn’t have any energy. I called in sick that day, but it continued. The times I went to work, I could not get through the day without lying on the floor and taking a nap. I couldn’t read the computer. My eyes could not focus, and I could not remember things. When I went to see a patient, I could not remember what I was seeing him for. So, I had to retire because it was unethical for me to continue. With these issues continuing for three years, the doctor diagnosed me with Postural Orthostatic Tachycardia Syndrome, which is also calls POTS and is being related to long COVID, so this obviously is a vaccine injury.
So, I started hanging out with a group in town called Health Freedom Information, and it was there that I started learning about how unsafe these vaccines were, once I had the vaccine injuries.
We wish the best for Sol, and others, and hope that a long-COVID off-button is discovered very soon. Perhaps it’s on the way: Dr. Mercola highlighted a potential off-button in this study by Dr. Peter McCullough.
Debunking Two Seattle Doctors Claims That “Unvaccinated” Are More at Risk of Myocarditis
For the first two years of COVID-19 shot rollout, reports finally surfaced proving the CDC hid evidence of myocarditis following the jabs.
For starters, documents obtained by Children’s Health Defense via a Freedom of Information Act request to the Center’s for Disease Control and Prevention (CDC) reveal that Pfizer and the CDC withheld evidence that COVID-19 vaccinations were causing myocarditis. The documents were revealed on March 16, 2023 by Project Veritas.
The Defender had earlier published an article on the topic on October 25, 2022.
Two months after COVID-19 vaccines were rolled out to the U.S. public, a statistically significant vaccine safety signal for myocarditis in males ages 8 to 21 appeared in the Centers for Disease Control’s (CDC) Vaccine Adverse Event Reporting System (VAERS) — but CDC officials waited another three months before alerting the public, according to a new study.
Over the past year, the CDC is finally admitting a causal connection between myocarditis and the COVID-19 shots. At the same time, they downplay the risk.
This spin doctor approach has trickled down to the Washington Department of Health with its latest ploy being an interview published on a DOH blog with two doctors: Dr. Sathish Mallenahalli Chikkabyrappa, pediatric cardiologist at Seattle Children’s, and Dr. Anita Chopra, internal medicine physician at UW and its Long COVID clinic.

Let’s review the answer to the first question:
Can COVID-19 infection cause myocarditis?
Dr. Chopra: Yes, and if you’re unvaccinated, it’s a significant risk. Getting at least one dose of the COVID-19 vaccine cuts the risk of myocarditis from COVID-19 infection in half.¹
Studies have found that unvaccinated patients with COVID-19 were 16 times more likely to develop myocarditis than patients without COVID-19.
Let’s examine those two claims.
Does the data (as opposed to the authors interpretation of the data) in the August 2022 paper that he cited support the claim that getting at least one dose of a COVID shot cut the risk of myocarditis? The study design muddies all results. What do you think?
Every single person in the study had received at least one vaccine. There were NO non-vaccinated individuals.
“Of the 42,842,345 people in the study population, 2,861 (0.007%) were hospitalized or died from myocarditis during the study period”
The study period was between December 1, 2020, and December 15, 2021.
The study window — meaning the only cases of myocarditis they assigned to either infection or vaccination were those that occurred within 28 days post vaccination or post infection.
The authors admit is was an assumption that myocarditis following exposure to infection or vaccination would be limited to 28 days.
Of the 2,861 people in the study who were either hospitalized or died from or with a myocarditis diagnosis, 114 tested positive for COVID prior to being vaccinated. And again, everyone was vaccinated. This means they vaccinated 114 COVID positive individuals.
Of the 2,861 myocarditis hospitalizations or deaths, 617 had received a COVID shot within 28 days of diagnosis.
“Of the 5,934,153 patients with a SARS-CoV-2 infection, 195 (0.003%) were hospitalized or died with myocarditis in the 1 to 28 days after the positive test; 114 (58.5%) of these events occurred before vaccination.”
So the study data shows within a 28-day window following either infection or vaccination, 617 cases occurred following vaccination and 114 occurred following infection, and for 81 cases the person was vaccinated and then diagnosed with COVID in a 28 day window.
Of the 2,861 myocarditis hospitalizations or deaths, there were 2,049 outside of the 28-day window. Again, everyone in the study had received at least one COVID shot. Did infection or vaccination play a role in the 2,049 hospitalizations or deaths? What about the known fact that spike protein is generated by shot recipients’ cells longer than 28 days? What about the phenomenon of vaccine shedding exposure?
So what do you think? We encourage you to read the full study very closely. The study authors do make one concession, regarding the safety claim for young men: “However, the risk of myocarditis after vaccination is higher in younger men, particularly after the second does of the mRNA-1273 vaccine.”
Also calling into question their claim of efficacy, the paper cited often uses the same kind of Relative Risk calculation that Dr. Fauci used when claiming 95% COVID shot efficacy, when Absolute Risk should be used to help people weigh their risk exposure.
Expanding on this last point, it is unclear what data they used to make this claim. We think they might have cited that while 195 (0.003%) of nearly 5.9 million positive for a COVID infection were hospitalized or died within 28 days, 114 (58.5%) occurred before vaccination. Do you see how the percentages switched scales right in the middle of the results explanation? And even the 0.003% figure sounds a little frightening. But what is that if compared in an absolute risk calculation?
(Yep, we’re gonna do some math). 195 divided by 42,842,345, then times 100 equals 0.00045%. Or 4.5 per million. 114 before vaccination is 0.00027, or 2.7 cases per million. Looking at the difference, does 1.8 cases per million seem like a significant risk? The paper does mention absolute risk calculations, and their comparison is 35 per million myocarditis cases from an infection before vaccination, versus 23 per million if you’re vaccinated. So a difference of 12 cases of myocarditis per million if you’re infected before vaccination. That still isn’t cutting your risk in half. And this only pertains to the limited 28 day window.
As for the claim that “Studies have found that unvaccinated patients with COVID-19 were 16 times more likely to develop myocarditis than patients without COVID-19” — what is he actually saying? What patient pool is he referring to? What studies? If you can make sense of the statement, please let us know.
The topic of myocarditis in young adults was raised during the answer to the next question:
Can the COVID-19 vaccine cause myocarditis?
Dr. Chopra: Yes, but the risk is very low. For example, in people assigned male at birth age 12–15, the risk of developing myocarditis from a dose of the Pfizer vaccine is 0.007% — that’s 7 in 100,000. In people assigned male at birth age 16–17, the risk is 0.01%, or 1 in 10,000.² The risks are even lower among people assigned female at birth.
Dr. Chikkabyrappa: My team led a study that produced similar results — the COVID-19 vaccine is extremely unlikely to cause myocarditis.
Dr. Chopra: The key thing for people to understand is that the risk of myocarditis from vaccination is much lower than the risk of myocarditis from COVID-19 infection.³
Dr. Chopra uses the following link from the CDC to support this last claim:
How might the following exclusion criteria impact the study results? “Vaccine doses specifically coded as booster or extra doses were excluded. Persons with a positive SARS-CoV-2 test result ≤30 days before receipt of an mRNA COVID-19 vaccine were excluded from the vaccine cohorts; persons who had received an mRNA COVID-19 vaccine dose ≤30 days before a positive SARS-CoV-2 test result were excluded from the infection cohort. In the infection cohort, there were no other exclusions based on vaccination status.”
As much as the two doctors believe that the risk of myocarditis for children is low following the COVID-19 shots, they again do not mention that it is still higher for vaccinated children than it is for those children who do not receive the jab, as stated in a study done this past May 5. As reported in the Epoch Times, the study said that myocarditis and pericarditis only occur after vaccination and not after COVID-19 infection, according to a recent preprint led by researchers at Oxford University, which compared health outcomes among COVID-vaccinated and unvaccinated children.
“Whilst rare, all myocarditis and pericarditis events during the study period occurred in vaccinated individuals,” the authors wrote.
Since Dr. Chikkabyrappa pediatric is a cardiologist at Seattle Children’s Hospital, he could be referring to the following study reported in The Defender on March 29, 2022:
A new peer-reviewed study shows more than two-thirds of adolescents with COVID-19 vaccine-related myopericarditis had persistent heart abnormalities months after their initial diagnosis, raising concerns for potential long-term effects and contradicting claims by health officials that the condition is “mild.”
Researchers at Seattle Children’s Hospital reviewed cases of patients younger than 18 years old who presented to the hospital with chest pain and an elevated serum troponin level between April 1, 2021, and Jan. 7, 2022, within one week of receiving a second dose of Pfizer’s vaccine.
While 35 patients fit the criteria, 19 were excluded for various reasons. Cardiac magnetic resonance imaging (MRI) of the remaining 16 patients was performed three to eight months after they were first examined. The MRIs showed 11 had persistent late gadolinium enhancement (LGE), although levels were lower than in previous months.
According to the study, “The presence of LGE is an indicator of cardiac injury and fibrosis and has been strongly associated with worse prognosis in patients with classical acute myocarditis.”
Dr. Chikkabyrappa then added the following:
And, the rare cases of myocarditis caused by the COVID-19 vaccine are more mild and more likely to resolve on their own than myocarditis caused by COVID-19 infection. A lot of the unvaccinated children we saw required hospitalization and ICU treatment for COVID-19-related myocarditis.
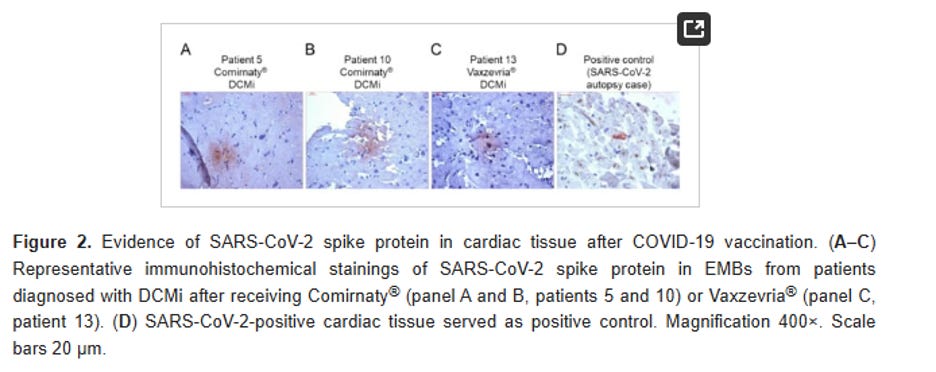
As for this comparison of severity, the interviewer did not ask him about a study done in which tissues were taken from heart cells, which said the following:
In the present cohort, the SARS CoV-2 spike protein was found to be expressed on cardiomyocytes in 9 of the 15 patients. Thus, vaccine-encoded spike protein seems to reach the heart, where it might trigger inflammatory response, resulting in the development of myocarditis or DCMI.
Although causal relationship between and the occurrence of myocardial inflammation cannot be established based on the findings, the cardiac detection of spike protein, the CD4+ T-cell-dominated inflammation and the close temporal relationship argue for a vaccine-triggered autoimmune reaction.
The following slides show more spike protein damage to the heart from the COVID-19 shot than a natural infection.
Getting back to the myocarditis risks for children, the question of them playing sports came up:
What about children who play sports — are they at higher risk for myocarditis? Should they still get the COVID-19 vaccine?
Dr. Chikkabyrappa: Yes, they should get the vaccine. There is no evidence to suggest that playing sports increases the risk of myocarditis from COVID-19 vaccination. A child is much more likely to develop myocarditis from a random viral infection than from the vaccine. Treatment and recovery for children are the same as for adults: rest, proper hydration, and NSAIDS, like ibuprofen.
If that is the case that a child is more likely to develop myocarditis from a random viral infection than from the COVID-19 shot, then why have the incidents of athletes collapsing on the field from myocarditis been occurring so often ever since the rollout of the shots in 2021? In her book, COVID-19 Vaccines and Beyond, Sally Saxon gave the following evidence:
The International Olympic Committee studied data from 1966 to 2004 and found an average of 29 deaths per year worldwide of athletes under 35 years old.[footnote 245] However, between the COVID vaccine rollout and mid-November 2022, at least 1,502 athletes have collapsed, of whom 1,029 have died.[footnote 246] In the vaccine’s first 20 months (1.66 years), that is an annual average of 510 athlete deaths, which is an increase of nearly 18X or 1,800%.
Sally Saxon also gave the following reference in her book Vaccines and Beyond.
In her book, Neither Safe Nor Effective: The Evidence Against the COVID Vaccines, Dr. Colleen Huber reports on her interviews with two sports coaches who each worked with a group of 20 student athletes.[footnote 247] Fifteen were high school age and the rest were younger. The students had spoken openly and freely about their vaccination status, and how they felt after receiving the shots. Half were vaccinated, and half were not. The coaches had to speak under conditions of anonymity, for obvious reasons. The coaches found the following: with regard to the vaccinated students:
None were competing at their own previous levels, and were even worse than in 2020.
None demonstrated their previous endurance during exercise drills.
Recovery times were longer than before, and longer compared to the other students.
Most or all complained of at least one of the following: “a) chest pain; b) dizziness; c) seeing stars; d) feeling faint; and e) shortness of breath;”
“Unvaccinated girls are now beating vaccinated boys in a competition, whom they could not do well against last year.”
Most of the above symptoms were still evident in all of the vaccinated athletes even several months later.
Unvaccinated students did not experience any of the above symptoms or declines in their performance or endurance, but continued to improve. According to Huber, the above information came solely from spontaneous remarks by the students themselves, with no prompting from the coaches as to symptoms they were experiencing.
In the interview, Dr. Chopra also downplayed the risks of the COVID-19 shot by saying, “Most cases of vaccine-related myocarditis are self-limiting, meaning they resolve on their own.”
This claim was also made at the latest ACIP meeting, as reported by The Defender:
The presenter, the CDC’s Dr. Lakshmi Panagiotakopoulos, also said in the presentation that vaccine-related myocarditis, a known risk, resolved quickly.
Karl Jablonowski, Ph.D., a research scientist at Children’s Health Defense, told The Defender that this was an error:
The longest study of vaccine-induced myocarditis shows that it does not act like other forms of myocarditis. The scar tissue persists much longer in the vaccinated — so long that the longest study of patients wasn’t long enough to actually see the scar tissue resolve.
A March 29, 2024 article in ZeroHedge further drove this point home about persistent scarring in the heart following the COVID-19 shots:
Heart scarring was detected more than one year after COVID-19 vaccination in some people who suffered myocarditis following receipt of a shot, researchers reported in new studies.
A third of 60 patients with follow-up cardiac imaging done more than 12 months after their myocarditis diagnosis had persistent late gadolinium enhancement (LGE), which is, in the majority of cases, reflective of heart scarring, Australian researchers reported in a preprint of a new study, published on March 22.
The median time from receipt of a vaccine to follow-up imaging was 548 days, with the longest interval being 603 days.
“We found that the incidence of persistent myocardial fibrosis is high, seen in almost a third of patients at >12 months post diagnosis, which could have implications for the management and prognosis of this predominantly young cohort,” the researchers wrote.
“The long-term clinical implications of LGE in this condition are as yet unknown, but LGE has been demonstrated to confer worse prognosis in non-COVID-19 vaccine-associated myocarditis, especially if it persists beyond six months,” they added later, pointing to several previous papers.
A paper published January 24, 2024 by Peter McCullough, Stephanie Seneff, Jessica Rose, M. Nathanial Mead, Steve Kirsch, and others said the following on page forty-one:
In adolescent males, however, myocarditis can have a mild outward clinical appearance yet result in severe cardiac fibrosis (scarring), with permanent damage to the heart muscle [274,275]. Such damage can eventually lead to congestive heart failure and death many years later [276]. The registrational trials were insufficient for detecting these long-range hazards, most of which only became evident after 2.5 years of follow-up observation and over a billion mRNA injections.
Finally, we guide you to one of our favorite medical freedom authors and news source – Jennifer Margulis and her Vibrant Life Substack for her timely article:
How to Avoid Vaccine-induced Myocarditis (July 1, 2024) which also talks about POTS.
In conclusion, there are so many doctors and scientists who are sounding the alarm about myocarditis related to COVID shots, if they were doing their medical due diligence, the doctors interviewed by the DOH would be reading broadly and deeply and seeing that the evidence against the shots is overwhelming.
And why is DOH only considering myocarditis as a vaccine injury concern? What about vast array of reported adverse events following the shots that include such things as POTS, ischemic stroke, pregnancy loss, autoimmune disorders, blood clots, permanent disability?
New Washington State Voter Guide is Published
Stand for Health Freedom, our national affiliate group, has conducted surveys of Washington candidates for office in the 2024 primary election and consolidated their endorsements on this 1-page flyer you can share with neighbors, friends and likeminded organizations. Of course, research candidates on your own, but this will give you a good head start to look for those candidates who Stand for Health Freedom.

The (inaugural) Guano Report
In this movement, we often feel pressure from internal (and external) forces to relieve ourselves from the mess. The Bird Flu narrative being pushed by the world’s health organizations is one such source of pressure we’d just like to release. That’s what the Guano Report is all about. A place where we can talk about all this excrement.
First, we leave you with a gross pile of bureaucratic excess where the BARDA has just awarded Moderna an exorbitant $176M to advance an H5Nx bird flu toward production.
Second, we remind you that actual, non-gain of function bird flu viral particles are easily wiped up if you take the EFU Challenge. No fuss, no mess, just a little natural anti-viral substances in your breathing apparatus and virus particles inactivated.*
*There is no guarantee that the compounds referenced in the EFU Challenge will knock out gain-of-function, frankenvirus particles until they are accidentally/on-purpose released into circulation and tested. However, if mankind ever creates a virus that can’t be inactivated by iodine or H2O2, it would likely be so lethal it would not spread far. Or if intentionally spread through artificial means, it would wipe out all of humanity. But let’s pretend the gain-of-function enthusiasts are not that stupid.