


ICWA Weekly News 9-4-24
EpiPens ordered for all schools - why so many allergies? Healthcare workers still pressured to take COVID shots; More 🐓 Guano 💩 Report: 🐄 Testing and new animals blamed for new/old virus

In this issue:
Standing Order for EpiPen in Washington State Schools
DOH’s Power of Providers Step up COVID-19 Shot Campaign on Healthcare Workers
🐓 Guano 💩 Report 🐄: Vaccine Testing begins in Cattle; and lethargic jungle animals are now being blamed for flu-like symptoms
August 30 Episode of Informed Life Radio - - Notes and Links
Health Hour: Eat This, Not That
Guest: Dr. Michael Gaeta
https://michaelgaeta.com/
https://www.westonaprice.org/
Liberty Hour: Evidence of Capture
Capture of every Immunization director/manager in every state in the U.S.: https://www.immunizationmanagers.org/corporate-alliance/
https://www.cms.gov/medicare/enrollment-renewal/special-needs-plans/model-care
Sugar Industry https://www.usatoday.com/story/news/nation-now/2016/09/13/study-how-sugar-industry-lied-heart-disease/90307932/
NCQA (sellers of HEDIS measurement system) is a $100M non-profit that pays its top executive Margaret O’Kane over a $1M per year. Form 990: https://beta.candid.org/profile/7755114
The President’s 2024 CDC Budget highlights regarding infectious diseases (aka vaccines): $1.25B for immunizations (+37% increase yr-over-yr), $764M for global infectious disease, $1B for Pandemic Preparedness, $6B mandatory for Vaccines for Children, $1B vaccines for adults vaccines; and another $6B for pandemic preparedness.
Meanwhile, the NIH has a $48B budget.
Revolving door is not new. Note Sam Skinner’s role as U.S. attorney tasked with investigating makers of Aspartame, recuses himself but then get’s hired by Aspartame’s law firm, then becomes Secretary of Transportation. https://en.wikipedia.org/wiki/Aspartame_controversy
Peter Doshi, editor at the British Medical Journal, who is somehow allowed to publish critical articles, points out the acceptability of “behind the scenes” influence government decisions and policy, and the story of Doran Fink, a senior FDA covid vaccine approver who took a job with Moderna.
Dr. Julie Gerberding’s blessed path to retirement CDC >> Merck >> Cerner (bought by Oracle) >> Wellcome Trust initiative >> FNIH
https://www.merck.com/news/dr-julie-l-gerberding-to-retire-from-merck/
Cerner, bought by Oracle in 2022, Dr. Gerberding made about $1.25M in stock sales from her time as director, on top of her annual 2021 board member compensation of $328,535.
FNIH: WTF is the FNIH? Somehow, another federal health agency needs a ‘foundation’ to launder money – the Foundation of the National Institutes of Health. And who is a full-time board member making a $325k salary in ‘retirement’? Julie Gerberding
Standing Order for EpiPen in Washington State Schools
Last Wednesday, August 28, the Washington Department of Health’s (DOH) Office of Immunization sent out a notice of a new standing order from the Secretary of Health that would allows schools to prescribe epinephrine to schools and school nurses.

Katherine Graff from the Office of Immunization wrote the following:
This standing order is issued under RCW 43.70.827, which authorizes the Secretary of Health or the Secretary's designee to issue a statewide standing order prescribing epinephrine to any school district or school for use by a school nurse or other designated trained school personnel.
Any Washington school district or non-public (private) school may obtain a supply of epinephrine under this standing order to keep and administer as needed at any school. You can use stock epinephrine on school property, including: school buildings, playgrounds, school buses, and field trips or sanctioned excursions away from school property following district or school policy and procedure and subject to the requirements of this standing order.
Schools are not legally required to stock epinephrine. However, this standing order allows for more consistent epinephrine access in schools.
Schools can access the epinephrine standing order and FAQs about the standing order on the DOH Schools web page.
This ability for a standing order by the Secretary of Health to prescribe Epi-Pens was contained in HB 1608 Expanding access to anaphylaxis medications in schools, which passed in the 2024 session, updating existing Epi-Pen law from 2013, which states:
Findings—2013 c 268: "(1) The legislature finds that allergies are a serious medical disorder that affect more than one in five persons in the United States and are the sixth leading cause of chronic disease. Roughly one in thirteen children has a food allergy, and the incidence is rising. Up to forty percent of food-allergic children may be at risk for anaphylaxis, a severe and potentially life-threatening reaction. Anaphylaxis may also occur due to an insect sting, drug allergy, or other causes. Twenty-five percent of first-time anaphylactic reactions among children occur in a school setting. Anaphylaxis can occur anywhere on school property, including the classroom, playground, school bus, or on field trips.
What are the stats now? CDC says, as of 2021, more than 1 quarter of adults and children in the U.S. have at least one allergy. So we went from more than 1-in-5 to more than 1-in-4 in less than a decade. Peanut allergies are noteworthy since many schools simply don’t allow PBJ sandwiches anymore. CNBC reported on a study from the Jaffe Food Allergy Institute at New York’s Mount Sinai hospital and found that from 1997 to 2008, peanut allergies tripled from 1-in-250 children to 1-in-70. What’s going on? “Experts are stumped.” according to the authors.
The elephant in the room not being addressed is why. Why are the immune systems of Americans increasingly messed up? We know many of those answers (immune-skewing vaccines, immune-suppressing drugs, environmental toxins destroying gut biomes, etc.).
Could allergies be related to vaccinations, which have been administered in exponentially increasing amounts? ICWA and many other organizations suspect that it is related and that data should raise that specific alarm, beginning with the Mawson study of 2017 where allergic rhinitis (hay fever) was 30 times higher in vaccinated children than in the study’s unvaccinated kids.
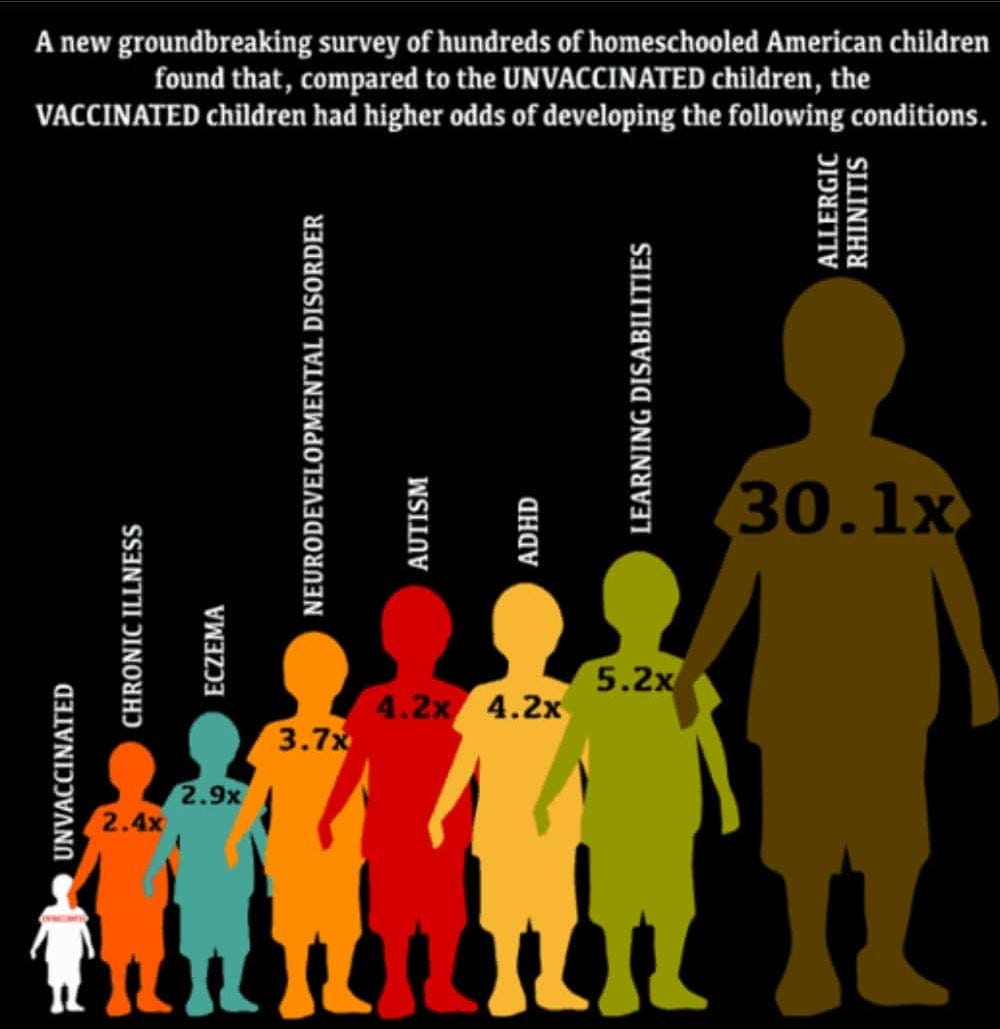
As often cited by the medical freedom movement, this study also found many other chronic conditions to be magnitudes higher in the vaccinated population, adding to the calls for the CDC and NIH to do an honest vax/unvax study. Our legislatures and public health agencies steadfastly refuse to address the elephant as doing so would undermine the very foundations of the current corrupt captured political and medical-pharmaceutical systems.
Regardless of how we got here, Epinephrine has been very effective as an emergency treatment for life-threatening allergic reactions. Also known as adrenaline, epinephrine is a hormone and neurotransmitter. It is most popularly marketed under the trade name EpiPen. Drug.com says the following about it:
EpiPen and Epipen Jr are used to treat life-threatening allergic reactions (anaphylaxis) to insect stings or bites, foods, drugs, and other allergens, and also treat exercise-induced anaphylaxis. EpiPen Auto-Injectors reduce wheezing and improve low blood pressure, hives, severe low blood pressure, and other symptoms of an allergic reaction.
ICWA Director Lisa Templeton noted the windfall this order represents for Big Pharma.
When I was a health tech at Kent School District, my school had several students with EpiPen orders. Their parents were required to provide the injections to us to keep in the nurse’s office, and we were to administer it only to the prescribed student if needed. The district did not have the option to purchase the products to have on hand for anyone who might present with symptoms. This new standing order will result in revenue increases for EpiPen manufacturers--at taxpayer expense.
How ironic is it that this increased need to be prepared for anaphylactic reactions is occurring along with the increased vaccine uptake being ‘recommended’ by the CDC and FDA, and promoted by the DOH’s Office of Immunization, which has included the COVID-19 shots for nearly four years. These policies are not without dangers.
VAERS shows 9,208 reports of "anaphylactic reaction" following the COVID-19 jabs.
As we always like to point out, these are the reactions that are being reported. A 2011 HHS-sponsored study estimated that “fewer than 1 percent of vaccine adverse events are reported” to VAERS. Put another way, VAERS could be missing as much as 99% of vaccine injuries.
Fifty-nine of those anaphylactic reactions from the COVID-19 shots have occurred here in Washington.

VAERS ID: 1394280 was for a twelve-year-old female. The write-up reported “anaphylaxis, trouble breathing, throat swelling” on the same day of taking the Pfizer shot.
Here in Washington, VAERS also shows ninety-eight cases of anaphylactic reaction following any vaccination.

Besides the aforementioned reaction to the COVID-19 shot, three anaphylactic reactions have occurred in school-aged patients in Washington following vaccination. They are as follows:
VAERS ID: 316424
Submitted write-up for this six-year-old female: Patient had coughing and gagging within minutes of Hep A and VZV vaccines. Within 10 minutes had wheezing and urticaria all over her body and respiratory compromises. Given 20mg of Diphenhydramine IM. Ambulance arrived and taken to ER. Patient had severe angioedema almost requiring intubation but resolved with epinephrine and Solumedrol. Admitted to hospital for continued treatment and discharged after 24 hours on steroids, antihistamines and EpiPen. Will also see allergist. 7/17/2008 MR received for DOS 6/2-/2008 with DX: Allergic reaction with angioedema and anaphylaxis. Patient presented to ER from MD''s office . Patient developed hives, breathing and swallowing difficulty, rash, itching and swelling which began just after receipt of Hep A and Varicella vax. PE (+) for facial angioedema, muffled voice, drooling and urticaria. Sx resolving with Epi, Benadryl, solumedrol. Admitted o/n for observation.
VAERS ID: 424986
Submitted write-up for this ten-year-old male: Patient received MMR #2 on 5-26-11 at 1:00pm. Mom states patient started sneezing repeatedly at 1:45pm, after leaving the office. Mom states EMS activated, EPIPEN administered & BENADRYL given at 2:00pm due to s/s of anaphyl. widespread hives, SOB, cough, (R) ear, lip edema.
VAERS ID: 892396
Submitted write-up for this seven-year-old male: 5 minutes after receiving vaccine: patient experienced shortness of breath, coughing, difficulty breathing, full body hives, welt/blister at injection site. 20 minutes after receiving vaccine: ER diagnosed and treats patient for anaphylactic reaction to flu vaccine.
While increased need for Epi-Pens is a tragic reality, the same can’t be said for other drugs included in SB 6095, which also passed in 2024. ICWA strongly opposed the “Establishing clear authority for the secretary of health to issue standing orders” bill because of its open-ended nature to expand medication access. Its passage has given the Secretary of Health the power to “issue a prescription or standing order for any biological product, device, or drug for purposes of controlling and preventing the spread of, mitigating, or treating any infectious or noninfectious disease or threat to the public health. Any such prescription or standing order is issued for a legitimate medical purpose.”
Really . . . we need more access to medications? We are the most medicated country in the world.
The DOH said this law was for COVID-19-like emergencies and for overdose medication, but they asked for, and got, a general standing order power for any medication or measure they see fit to prescribe. It’s another very concerning step toward centralizing power, a not-so-slow creep toward eliminating the autonomy of all doctors to actually practice medicine and make individual medical judgements in the best interest of their patients. It won’t be long until our legislature passes a Kiosk and Drone bill, bypassing doctors altogether, letting AI prescribe, deliver, and inject, all without anyone doing any critical thinking.
Power of Providers Step up COVID-19 Shot Campaign on Healthcare Workers
On that same Wednesday, August 28 that the Department of Health (DOH) had issued its standing order for EpiPen, the DOH was also using its Power of Providers (POP) initiative to further convince healthcare providers to, in turn, convince their patients to take more COVID-19 shots.

Naturally, the POP announcement began with a nice, cordial tone:
Dear Healthcare Partners,
We are emailing today to give you an update on the 2024-2025 COVID-19 vaccine. The CDC recommends everyone 6 months and older should get an updated 2024-2025 COVID-19 vaccine.
As of August 22, 2024, the FDA Approves and Authorizes Updated 2024-2025 mRNA COVID-19 Vaccines. The 2024-2025 mRNA COVID-19 vaccines have been updated to more closely target currently circulating variants and provide better protection against serious consequences of COVID-19, including hospitalization and death.
But why has the government changed its messaging? Remember when Tony Fauci said the following on MSNBC about the COVID-19 jabs?
“The situation is so clear. The data confirm that if you get vaccinated, you are protected, even with the Delta variant.”
Also, Fauci: If You’re Vaccinated, You’re Safe. If You’re Not, You’re At Risk (youtube.com)
We even heard the same thing from President Joe Biden during a Town Hall meeting:
“You’re not going to get COVID if you get these vaccinations.”
Finally, 10 Times “Experts” LIED About COVID (And We Have RECEIPTS) (youtube.com)
But nowadays, as in this case with the POP announcement, the COVID-19 shots only “provide better protection against serious consequences.”
In this case, this damage control technique is called “changing the goalposts,” and, as noted by Suzanne Humphries in her book Dissolving Illusions, is nothing new:
When it was clear that the smallpox vaccine was not able to prevent disease, the medical profession tried to justify vaccination by changing the goalposts from lifelong “perfect” immunity to “milder disease.” Similar dogma is repeated in 2013 to justify the fact that pertussis and influenza vaccines don’t protect recipients either. But did smallpox vaccination really decrease the death rate and make for a milder disease?
In the 1844 smallpox epidemic, about one-third of the vaccinated contracted a mild form of smallpox, but roughly 8 percent of those vaccinated still died, and nearly two-thirds had severe disease.
A letter to a newspaper in 1850 claimed there were more admissions to the London Small-Pox Hospital in 1844 than during the smallpox epidemic of 1781 before vaccination began. The author also noted that one-third of the deaths from smallpox were in people who had previously been vaccinated.
Letter to the newspaper:
Daily experience now unhappily shows an altered state of things: small pox, in spite of vaccination, is rapidly on the increase… There were more admissions to the London Small-Pox Hospital in 1844 than in the celebrated small-pox epidemic of 1781 before vaccination was introduced. I shall also select the Registrar’s returns of one of the country districts (Bradford) to show how little protection vaccination afforded in the last quarter of that year, 1844: deaths from small-pox were recorded, 60, or nearly one-third, of which had been vaccinated.
The POP announcement also provided no documentation on the following claim:
People who are up to date on their vaccinations have lower risk of severe illness, hospitalization, and death from COVID-19 than people who are unvaccinated or who have not completed the doses recommended by the CDC.
This claim was first refuted by a Cleveland Clinic study in June 2023.
The summary in the study’s abstract says it all:
Among 48 344 working-aged Cleveland Clinic employees, those not “up-to-date” on COVID-19 vaccination had a lower risk of COVID-19 than those “up-to-date”. The current CDC definition provides a meaningless classification of risk of COVID-19 in the adult population.
Then last February 3, the Epoch Times referred to a narrative review that COVID-19 boosters could be doing more harm than good. The article began as follows:
Frequent administration of mRNA COVID-19 boosters may impair the immune system response in immune-compromised individuals, raising questions about whether giving multiple vaccine doses is more harmful than beneficial.
According to a narrative review published on Jan. 27 in Clinical and Experimental Medicine, repeated COVID-19 vaccination may increase the likelihood of experiencing SARS-CoV-2 infection and other pathologies. Additionally, receiving multiple doses may result in much higher levels of IgG4 antibodies and impair the activation of white blood cells that help to protect the body from infections and cancer.
The POP announcement then revealed its reliance on the CDC:
The Washington State Department of Health is currently updating webpages and documents to align with the most recent CDC guidance.
How odd this is considering that the CDC released a study last April, as covered by the Epoch Times, showing that children who received an original COVID-19 jab have little protection against hospitalization just months after vaccination.
An Epoch Times article noted the following:
Children initially have 52 percent protection against hospitalization but that estimated effectiveness plummeted to 19 percent after four months, according to the paper.
Protection against so-called critical illness also dropped sharply, from 57 percent to 25 percent, researchers found.
The researchers include CDC employees and the paper was published in the CDC’s weekly digest on April 18.
It’s staggering that DOH and CDC take the absurd stance that four months of decreasing protection would be worth the acknowledged risk of myocarditis, which causes lifetime complications and even death.
Staying true to form, the POP announcement ended with closure of “keep up the good work” cordiality to healthcare providers:
Thank you for all the work you are doing to keep our communities safe and healthy. Please don't hesitate to reach out with questions or feedback.
Power of Providers (POP) Team
Executive Office of Healthcare Innovation and Strategy
Washington State Department of Health
powerofproviders@doh.wa.gov
If you’re a provider, we encourage you to ask them about their claims.
🐓 Guano 💩 Report 🐄 + Lethargic Jungle Animals
Cattle tested as new Avian Flu vaccine passes through USDA approvals. BIO News covered the event noting:
What industry’s saying: Turkey, egg, and dairy producer associations wrote to Secretary Vilsack on Aug. 16 saying they urgently need a vaccine for livestock. Producers were previously hesitant on vaccines because vaccinated animals test positive for avian flu antibodies, which could mean they can’t be exported.
So, who came up with an antibody test as a criteria? That would mean an animal has either superior natural immunity or inferior vaccine-induced-antibodies. Either way, we are told antibodies mean protection which should = healthy animal.
But why let common sense get in the way? Just remove “unscientific barriers.”
Vaccination needn’t interfere with exports, according to John Torres, BIO Senior Director, Federal Government Relations, Agriculture & Environment: “We need to work with our trade partners to ensure that unscientific barriers to trade don’t arise from the need to address the health of farm animals and the safety of our food supply.”
Hang on a minute. We smell something, and it’s stronger than guano. Could it be that some of those “unscientific barriers” are we-the-people’s opposition to animal products from vaccinated animals, especially those injected with mRNA shots? That would explain using antibodies as the measure because then naturally immune and vaccinated animals would be barred from trade markets, putting ranchers between the proverbial rock and a hard place. Hmmm. How much you wanna bet that this is all leading to some sort of labelling regulation that makes it impossible for consumers to identify products from vaccinated animals?
Well, they’ve launched the vaccination campaign in the face of the unscientific barriers. This Guano Report predicts the USDA and FDA will quickly rubber-stamp all the approvals necessary to bring these products to market, since vaccines solve all respiratory infection ills. 🤮
In related news: 🦥 🦠
Feeling left out of all the animals in the news (swine, birds, cows, monkeys), and as per their reputation, the Sloth Fever virus has sluggishly made it into the news. And it must be serious since The Scientific American ran an article on its cause - the Oropouche virus. It is transmitted by midges, making it different from all the mosquito borne diseases with which our friend Bill Gates is now in the boxing ring.
Our photography team went on mission in the Amazon to verify the seriousness of the article. They were able to capture evidence of what’s causing this new outbreak, confirming our worst suspicions.

There are no vaccines yet for this virus that’s been known about for over 60 years, but they are called for in this March 2024 paper. With all this news, we’re certain another vaccine is on the way because…OneHealth!
Luckily, most sloths have safely built up antibodies to oropouche and live in harmony, like this happy little tyke.

What animal will be next? The hedgehog?