

ICWA Weekly News
ICWA Weekly News
Radio show links, Taxpayer-funded marketing of EUA Shots & Drugs, Florida protects people not Pharma, Myocarditis in WA


In this newsletter:
Radio Show links
Continued Taxpayer-Funded Marketing of COVID-19 Shots & EUA drugs earning billions for their makers
Florida Chooses Public Health Over Pharma Profit
Myocarditis in Washington Following COVID-19 Shots
May 19 Episode of An Informed Life Radio - show links
Guests: Sharon Hanek, Katherine Green
Gov. Inslee vetoes community notice for sexually violent predator relocation - MyNorthwest.com
Home - Children's Health Defense Oregon Chapter (childrenshealthdefense.org)
We The Patriots USA - When you stand up to tyrants, we stand UP for you.
Taxpayer Funded Marketing of COVID-19 Shots & EUA Drugs
It’s the perfect business model: Instead of implementing and financing their own marketing campaigns for pushing their Emergency Use Authorized (EUA) COVID-19 shots*** and EUA Drugs, drug companies Pfizer (COVID-19 shot & Paxlovid), Moderna (COVID-19 shot), Merck (LAGEVRIO™ aka molnupiravir), and Gilead (Veklury ak remdesivir) enjoy the financial benefits and substantial reach of federal and state public health agencies—including Washington’s—doing it for them, at taxpayer expense.
***While the FDA put forth documentation on Pfizer’s Comirnaty and Moderna’s Spikevax COVID-19 shots that gave the impression the products were licensed, the public was never given access to any “licensed” products. And now, the FDA has discontinued use of all those initial “primary” series shots, so there will never be licensed versions of those available. Only the EUA bivalent “booster” shots are being distributed. The bivalent shots were tested against a few mice and not put through any human trials before being authorized.
Government marketing of products comes with an added benefit for the drug companies: government agencies aren’t held to the same standards and regulations as the companies in their marketing language. They should be, especially in regards to EUA products because those regulations apply to everyone, but they are not. For instance, while Pfizer & Moderna cannot make any claim about the safety or effectiveness of their COVID-19 shots that they have not demonstrated in a valid study, the WA State Department of Health and CDC routinely market them as “safe and effective” even in pregnancy.
The Public Health Advisor from the Seattle and King County staff has first supplied the fear factor:
“The virus that causes COVID-19 is still spreading in our communities and continues to mutate and evolve over time. Although community immunity has increased over time from both vaccinations and infection, everyday people in King County still get sick with COVID-19. People are still regularly being hospitalized and even dying because of COVID-19, especially among those who are older and have underlying conditions.”
The Seattle and King County staff then promotes the COVID-19 shots:
“It is still important to take measures to protect yourself and your family from COVID-19, including staying up to date with the recommended vaccinations, staying home when sick, wearing a well-fitting, high-quality mask when in crowded spaces, testing when you have symptoms and getting treatment promptly if you are eligible (see below), and improving indoor air ventilation to reduce the risk of spread.”
That “(see below)” referenced above leads to information and a link to the only COVID-19 treatments that the NIH has authorized: all still under Emergency Use Authorization despite the emergency being declared over, and despite the availability of truly safe and effective licensed off-label alternatives, such as Nobel-prize winning Ivermectin.

These EUA drugs have proven to be ineffective and dangerous, yet highly profitable.
2022 Revenues
Pfizer’s COVID shot: $37.8 billion
Pfizer’s Paxlovid: $18.9 billion
Moderna’s COVID shot: $19.3 billion
Merck’s LAGEVRIO™ aka molnupiravir: $825 million
Gilead’s Veklury aka remdesivir: $3.9 billion
The Seattle and King County staff then devotes an entire section to getting the COVID-19 shots:
How to get the COVID-19 vaccine after the emergency declaration ends
The federal government purchased a large supply of COVID-19 vaccines that is predicted to last through the summer of 2023. COVID-19 vaccines will remain free to all people, even if they don’t have insurance, while the national vaccine supply lasts.
After the federal vaccine supply runs out later this year, COVID-19 vaccines will shift to the private market.
After the vaccines shift to the private market, we anticipate that the process for getting a COVID-19 vaccine will be like getting flu shots and other routine vaccinations:
Many healthcare providers and pharmacies will continue to offer COVID-19 vaccinations
COVID-19 vaccinations will continue to be free for children in Washington
COVID-19 vaccinations for adults will be covered by most private insurance, Medicare (“Apple Health”), and Medicaid/CHIP
People who are uninsured will be able to get free COVID-19 vaccinations at certain local pharmacies and community health centers
Most forms of private health insurance, including all Affordable Care Act-compliant plans, must continue to pay for COVID-19 vaccines given by a health care provider in their network, without charging the patient. People with private health insurance may need to pay part of the cost if an out-of-network provider vaccinates them.
Community Health Centers and Public Health Centers have vaccinations for uninsured and underinsured people, if they enroll as patients.
An e-mail to King County residents goes even further by providing the following recommendations:
CDC COVID-19 Vaccine Recommendations
Everyone aged 6 years and older should get 1 updated Pfizer or Moderna COVID-19 vaccine to be considered up to date.
Some people may get additional COVID-19 boosters:
People aged 65 years and older may get 1 additional COVID-19 updated (bivalent) booster dose 4 or more months after the 1st COVID-19 updated (bivalent) vaccine
People who are moderately to severely immunocompromised may get 1 additional COVID-19 updated (bivalent) booster dose 2 or more months after the 1st COVID-19 updated (bivalent) vaccine
Children aged 6 months to 5 years old may need multiple doses of COVID-19 vaccine to be up to date, including at least 1 updated dose of Pfizer or Moderna. It depends on the number of doses they've previously received at their age.
Please check with a healthcare provider if you have questions about how many doses you need.
The COVID-19 updated (bivalent) vaccines target Omicron variants that continue to circulate in our communities. The vaccine also targets the original strain of the COVID virus. People who stay up to date with all recommended vaccine doses have the best protection against severe COVID-19.
King County also has resorted to target-marketing by creating an illustrated activity book for children ages eight and younger to help “Provide information for local children, caregivers, and parents about getting vaccinated in King County.”
UGF-activity-book-EN.ashx (kingcounty.gov)
This is not the first time King County has provided such a book that targets children. A year ago, the Seattle Department of Education and Early Learning (DEEL) created a comic book titled Handbook for Health Heroes. It comes with a subtitle: Answers to Your Family’s Questions about COVID-19 Vaccines for Kids.
HandbookForHealthHeroes.pdf (seattle.gov)
The comic book used a question and answer format. The June 29, 2022 issue of ICWA Weekly News provided an analysis of each of the answers given in that book:
ICWA News & Views - Informed Choice Washington | ICWA
King County also devotes a web page called “COVID-19 Vaccination for Children and Teens.”
COVID-19 vaccination for children and teens - King County
To target the older population, King County has provided three new videos in which “We encourage older adults to get the updated (bivalent) COVID-19 booster.”
COVID-19 Updated Vaccines and Older Adults (English and Spanish) - YouTube
The e-mail sent out to King County residents went on to state the following:
“Pease share with the people age 50+ in your life who haven't gotten their booster. Adults age 50 and older are at higher risk for hospitalization, long-term symptoms (long COVID) and death if they get sick with COVID-19. More information: kingcounty.gov/vaccine.”
Not to be undone, the Tacoma-Pierce County Health Department is providing $30 gift cards to anyone receiving the COVID-19 shots in the month of May.
💵 Protect your... - Tacoma-Pierce County Health Department | Facebook
As part of its marketing campaign for Pfizer and Moderna, the Tacoma-Pierce County Department web site only mentions the COVID-19 shots for protection from the disease by falsely stating, “Vaccine is the most effective tool to protect yourself and your community from COVID-19. Everyone 6 months and older is eligible.”
COVID-19 Vaccine | Tacoma-Pierce County Health Department (tpchd.org)
Florida Chooses Public Health Over Pharma Profit
While no Washington government official has set out an alarm, warning, or even caution about adverse events from the COVID-19 shots, last February in Florida, Surgeon General Joseph Ladapo, M.D., Ph.D., issued an alert to the Florida healthcare sector and the public warning that COVID-19 mRNA vaccines caused a “substantial increase” in reports of adverse events in Florida.
Ladapo reported that in Florida, there was a 1,700% increase in VAERS reports after the release of the COVID-19 vaccine, compared to an increase of 400% in overall vaccine administration for the same time period.
In his letter to the CDC, he pointed to an excess risk of serious adverse events, including acute cardiac injuries.
In their response, the CDC told Ladapo that the reports of adverse events are rare and “Do not mean that a vaccine caused the event.”
CDC FDA Letter to FL Dept of Health 03.10.2023
At the bottom of the same paragraph in that letter, the CDC wrote the following:
Recent concerns about increased reports of cardiovascular events provide an instructive example of the need to do further analysis when increased reporting of an event occurs. Despite increased reports of these events, when the concern was examined in detail by cardiovascular experts, the risk of stroke and heart attack was actually lower in people who had been vaccinated, not higher.
Here is the link to the study that the CDC was referring to:
ICWA reviewed the study and have the following questions and concerns:
The study only looked at Major Adverse Cardiovascular Events (MACE) in patients with COVID-19 within the time range they define, so by design it does not assess risk of MACE following receipt of a COVID-19 vaccine outside of that infection scenario. The wordsmithed language of CDC’s letter implied otherwise. For decades, this has been the CDC’s modus operandi: their marketing communications do not match the science they cite.
Read the below study design excerpt carefully and think about it. The CDC and others have consistently refused to examine the 14 day window following receipt of COVID shots when looking at rates of health outcomes in the vaccinated vs not-vaccinated.
“Individuals were classified as fully vaccinated if they received ≥2 mRNA vaccines or 1 Johnson and Johnson vaccine ≥14 days before SARS-CoV-2 infection and as partially vaccinated if they received only 1 mRNA vaccine or their second mRNA or 1 Johnson and Johnson vaccine within 14 days of infection. Previous work suggests that COVID-19 vaccination may be associated with cardiovascular events within a few days. Although causality is unclear, we assess risk of MACE 14 days following last recorded vaccination to address this possibility and mitigate survivor bias.”
Only incidences of MACE following first “index” COVID infections were included. “We also did not consider SARS-CoV-2 reinfections following index illness”.
If the study had include those vaccinated who were in that 14 day window, or who experienced reinfections, would the data point to an entirely different conclusion?
The authors state: “we included patients aged 18 to 90 years who were initially infected with SARS-CoV-2 between March 1, 2020, and February 1, 2022”. Which means the non-vaccinated group who experienced MACE included some of the U.S.’s most unhealthy individuals with multiple comorbidities. This is often referred to as “dry tinder”, when a circulating infection first hits a population and the most vulnerable succumb. In March of 2020, before there were many cases or deaths in the United States, the CDC changed the rules for filling out death certificate for COVID only. This led to “dry kindling” deaths being reported as COVID deaths, rather than the underlying health issue that increased their risk of dying from ANY infection, which is how all other deaths are reported. It’s not the infection per se that is lethal, it’s the health-status of the patient that makes the infection lethal. The study authors acknowledge that most cases of MACE in those who tested positive (another rabbit hole of concern because of the unreliability of PCR tests) for COVID-19 were in those with health issues making them potential candidates for MACE.
Study says: “Patients with and without MACE had significant differences in comorbidities including previous MACE (29.1% vs 0.9%; P < 0.001), type II diabetes (33.9% vs 7.5%; P < 0.001), hyperlipidemia (50.7% vs 14.4%; P < 0.001), ischemic heart disease (40.6% vs 3.9%; P < 0.001), liver disease (4.0% vs 0.8%; P < 0.001), and obesity (29.4% vs 16.4%; P < 0.001).”
Authors acknowledge “Limitations include unmeasured confounding variables”.
The authors write: “Overall, MACE was observed among 13,948 patients (0.7%): 12,733 cases occurred among nonvaccinated patients (0.7% of these patients), 160 in partially vaccinated patients (0.7%), and 1,055 in fully vaccinated patients (0.5%).” So, even with their excluding important windows of time and reinfections, even with their multiple adjustments and including a period when those most at risk of a MACE caught COVID, the difference between nonvaccinated and those they considered fully vaccinated was only .2%.
Have any researchers reproduced this study, and examined ALL the data? For results of a study to stand and be relied upon as having any weight, it must be testable and repeatable.
Finally, the spike protein in the lab-created SARS-CoV-2 virus, and the spike protein created in the cells of a vaccinated person produced by the injected genetically altered mRNA, are different. But they are both manmade and capable of great harm. The shots, however, have additional harmful factors, including but not limited to:
the ability for the injected mRNA carrying lipid nanoparticle to bio-distribute to every part of the body, including the brain and heart and reproductive organs
the high volume of spike protein made in the cells of the vaccinated and the as yet undetermined length of time spike protein can be generated
the known toxicity of the shot ingredients, such as the lipidnanoparticles
the toxicity of the undisclosed ingredients that continue to emerge, such as contamination by the plasmids used to make the mRNA.
Claiming that a “lack of transparency only harms Americans’ faith in science,” Ladapo on May 10 wrote another letter to the CDC, this time calling on them to “publicly” explain twelve key issues related to the COVID-19 shot rollout.
(4) Florida's Letter to the CDC and the FDA Exposes Vaccine Quackery (substack.com)
Number four in the letter relates to myocarditis:

Myocarditis in Washington Following COVID-19 Shots
At the European Parliament COVID-19 Summit in Brussels, Belgium on May 3, PhD researcher Jessica Rose presented data from the CDC’s Vaccine Adverse Event Reporting System (VAERS). In the video, her presentation begins at the 7:11:224 mark, and at the 7:19:13 mark she says:
“This is my last slide, and it is probably the most important:
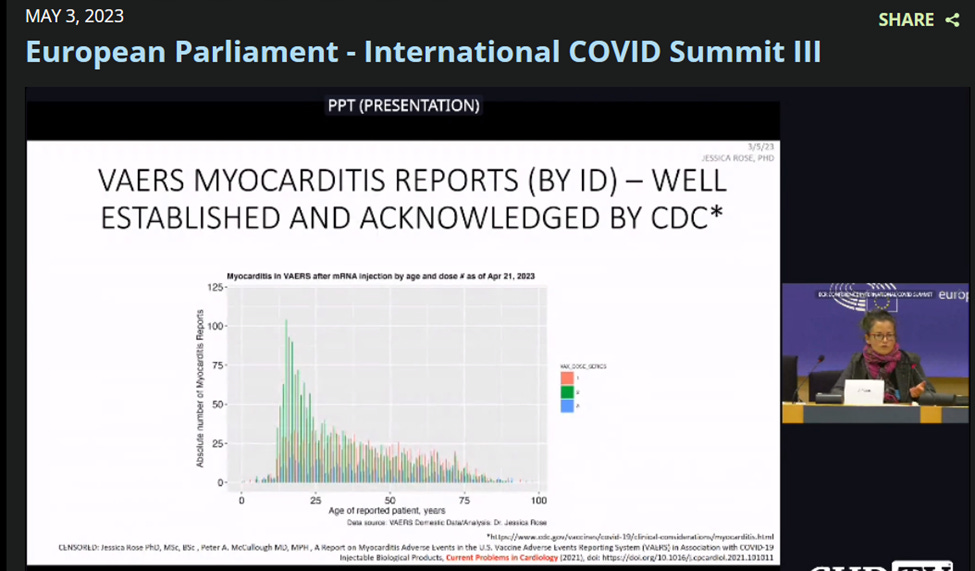
She went on to state the following:
It is well established and acknowledged, even by the CDC, that myocarditis is a problem in the context of these COVID-19 shots, inflammation of the heart. This slide is a chart that has been evident from the very beginning (of the rollout of the COVID-19 shots), and it remains evident in the way that I am showing. This is age on the X axis of all the reports pulled out of VAERS with myocarditis as an adverse event report, and the Y axis is just the absolute number, and the colors are by dose. So you can see following dose two there’s a much higher fold increase. It’s a much higher fold reporting rate for the second dose.
So that indicates that there’s evidence of causation. And I just also want to say that whenever I hear people repeating this mantra correlation isn’t causation I wonder if they ever heard of the Bradford-Hill Criteria, for this is the criteria that you can use to provide very solid evidence of causality from epidemiological data, and I’ve satisfied all ten.
European Parliament - International COVID Summit III | Childrens Health Defense
As of May 12, VAERS shows 16,864 cases of myocarditis were reported to the system in the United States and its territories with 132 of those cases occurring in Washington. As always, recall that VAERS suffers from under-reporting so the numbers can be used as safety signals only, not as the total cases actually occurring. Additionally, VAERS reports visible to the public are not updated, even when new information about worsening or additional symptoms or death are filed with the original report.
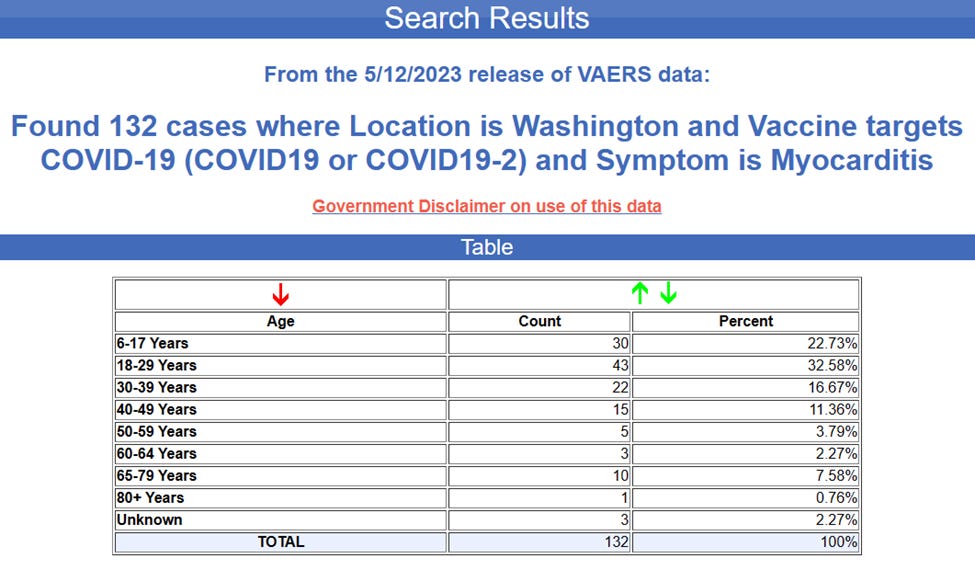
Ten of those cases in Washington were reported to VAERS in 2023, with nine of the cases being female.
The first case was reported on the January 1, 2023 of a twenty-three-year-old woman whose onset began fourteen days after taking her third dose of the Pfizer shot. The submitted write-up reads as follows:
I was hospitalized on 11/11/22 for chest pain and tachycardia. Cardiac CT and X Ray were normal, but troponin levels were elevated at .33 (about 3.5 times higher than normal). I had been feeling very weak and tired for ~3 days before the event. On the day of the event, I had gone on a bike ride (as usual, I am a cyclist and ride 3-5 times/week) and developed chest pain afterwards. As the pain worsened, my heart rate suddenly increased to 130 bpm for ~5 mins while I was at rest. I was short of breath during this time, and the pain was worse afterwards. I then decided to go to the hospital, where I was kept for 22 hours while they tried to determine what happened. Through process of elimination, I was diagnosed with mild peri- and/or myocarditis. My white blood cell counts were normal, but I had elevated inflammation markers and troponin.
VAERS ID:
A twenty-one-year-old female entered her report on April 18. Her onset of myocarditis occurred 713 days after taking a second dose of Moderna.
VAERS ID:
The ages for the other females with reports of myocarditis so far for 2023 are 37, 49, 55, 69, 72, 73, and 76. The one male report of myocarditis to VAERS for 2023 has been of a sixty-seven-year-old.
VAERS reports two Washington deaths after the onset of Myocarditis following the COVID-19 shots. Both deaths are of males.
The first was of a 35-year-old male whose onset began twenty-three days after taking a first dose of Pfizer.
VAERS ID:
Below is the submitted write-up:
DX: Myocarditis Onset of S/S 06/02/2021 S/S:Dyspnea on exertion, Fever/chills,Tachypnea Found to have acute basilar ischemic stroke, taken for emergent thrombectomy, but experienced progressive edema and ultimately tonsillar herniation. 35 year old man with medical history notable for likely untreated hypertension and tobacco use disorder who presented with reported fever, confusion, shortness of breath, and facial swelling, initially treated for allergic reaction/angioedema without effect, progressed to respiratory failure, found to have acute basilar ischemic stroke, taken for emergent thrombectomy, but experienced progressive edema and ultimately tonsillar herniation resulting in death. Regarding cardiac picture, patient with abnormal ECG, mildly reduced EF on echo (though could be due to untreated hypertension or to respiratory failure/critical illness), borderline troponin (need to check reference range). ED note initially mentions concern for myocarditis due to vaccine causing heart failure and subsequent respiratory failure, but appears this piece was written prior to MRI showing basilar stroke. Death note has myocarditis listed as a cause of death (among many), though a bit unclear if this was intentionally listed or just reflects a list of all hospital problems. Also had a CT of his head which showed scattered foci of gas within intraorbital soft tissues along with mild proptosis; unclear etiology for this (perhaps a fall with facial injuries prior to arriving at hospital?) Awaiting additional physician notes/imaging reports.
The other death was of a 62-year-old male after taking a second shot of Moderna.
VAERS ID:
Below is the submitted write-up from his daughter:
Chest pain & abdominal discomfort began 04/11/21 in AM, continued into afternoon. 911 was called, per my Dad they performed an EKG & vitals check, said everything looked ok but advised he go to ER. He called me (his daughter) to drive him to ER (ER only, no med facility attached), he was admitted to room where vitals showed aggravated hypertension, took MD 30 min to get into room to evaluate, no intervention meds given at that time. CT scan performed, showing aortic dissection, after which he was given nitroglycerin via IV and "gastric cocktail" oral solution. They had to plan transport to another facility as this location was only an ER, barely got him into an ambulance and leaving parking lot for transport when he went into cardiac arrest. Ambulance paramedics performed CPR for 10+ min without result, he was brought back into the ER where staff continued CPR another 15 min, spouse had to make choice to stop CPR as his aortic dissection was now such a low chance of success and due to lack of oxygen, per MD, less then 2% chance of neurological recovery. He had an autopsy performed which showed aortic dissection, massive cardiac arrest as well as myocarditis and enlargement of the heart, fluid around the heart. All data provided here is either from my first-hand witnessing in the ER (I am a trained Medic) or the actual autopsy report and ER medical records my stepmom & I obtained after his death. He was pronounced dead at 9PM on April 11th, 2021; approx 3 hours after admittance.
