


ICWA Weekly News 11-20-24
Petition against drinking water fluoridation discussed and declined by BOH; Debunking their bunk - More studies show cardiac events worse for COVID vaccinated vs infected; Support RFKJr. petition


*** Take our Survey on Friday: please look for our poll and vote for your favorite bill ideas***
In this issue:
Water Fluoridation Takes Center State at Washington Board of Health Meeting
More Debunking of the Claim That One Is More Likely to Get Myocarditis from COVID-19 Than from the Shots
Quick Action: Sign the Petition by SHF to show your support for RFK Jr. for Secretary of HHS. Make his appointment to big to rig.
November 15 Episode of Informed Life Radio - - notes and links
Health hour: Ozempic vs. Natural Satiety
Guests: Carol Grieve’, Mary Chantler. GLP-1 Agonists weight loss drugs, like Ozempic, are being intensely pushed and promoted, but are they safe? Holistic Health Coach Carol Grieve’ and Functional Nutrition Counselor Mary Chantler explain the risks of these drugs, especially for children, and how to stimulate satiety hormones in your body naturally.
Divine Integration Quantum Healing Hypnosis QHHT Functional Nutrition
Article: GLP-1 agonists like ozempic: how they work and how to get results without them
https://divineintegration.love/blogs/divinely-integrated-health-self/obesity
Liberty hour: Free Speech Fight
Guests: Alison Westover, Pete Serrano. When the Department of Natural Resources fired Alison Morrow, they violated her constitutional rights to free speech, free association, free press, as well as due process. Now, she’s fighting back against this injustice with a lawsuit by the Silent Majority Foundation.
Alison Morrow on Rumble
Water Fluoridation Takes Center State at Washington Board of Health Meeting
A personal account by Gerald Braude
As I peered around for a seat at the November 13 Board of Health (BOH) meeting in Tumwater, Board Chair Patty Hayes approached me and told me that Board Member Kate Dean, who also serves as my Jefferson County Commissioner, was not able to make the meeting because of the severe rainstorms on Highway 101. As it turned out, Dean appeared on Zoom. After we discussed that Dean was leaving the board because she decided not to run for reelection for county commissioner this year, Patty sighed and said, “And now we’re back to looking for another board member again.”
Video Link on TVW; which has a transcript option
details of Fluoride-related Petition Agenda Item 8
As she strolled away, I considered the many absentees during the meetings, at times leading to close calls of not having a quorum. Most conspicuous had been the absenteeism of Board Member Dr. Umair Shah, who was appointed Secretary of Health by Governor Jay Inslee after his reelection in 2020. Shah appeared at only one meeting this year, which was the August meeting in Seattle, and that was for just a few hours in the morning.
As I sat down a couple seats down the row from Bill Osmunson, we smiled to each other. I told him about all that national attention that water fluoridation had been receiving recently, including on The Highwire. He told me that he had been in contact with The Highwire staff. He then glared at the board members seated at their U-shaped table as he told me about his frustration with their silencing him for his petition to the board to recommend removing fluoride from all drinking water in the state, which would be heard at 1:30 pm. “They won’t give me a chance to refute what they say,” he said. “And they don’t know what they’re talking about.”
He then relaxed his shoulders, turned his look toward me, and said, “At least you folks already had a big win when the Board of Health voted not mandate the COVID-19 shots for school entry requirements.” I nodded and told him how hard ICWA had worked on that, how stressful that time in the winter of 2022 was for us, and how pleasantly surprised we were with the board’s unanimous vote.
Before we knew it, Bill was called up to the speaker’s table for his public comment. He told them at the get-go that the board’s job was to protect public health. He added that the State Board of Health is supposed to adopt rules necessary to assure safe water, and its rules don’t “Say a single thing here about assuring benefit.” He added the following: “That's the Food and Drug Administration's job, not your job. You're to take alleged claims of benefit and set them to the side. Your job is to look at safety. The National Sanitation foundation, the CDC, the FDA, the EPA, and three of the major fluoride manufacturers have all, when asked under threat of perjury in court, ‘Do you have one study on the safety of fluoridation to the human brain?’ all the authorities said no.” He then reiterated to the board what he had told me earlier: “We need a forum. I can't tell you stuff that needs to be learned in three minutes. This is not a forum.”
ICWA President Bob Runnells also spoke in support of Bill’s petition:
Speaking on behalf of our thousands of members across the state at Informed Choice Washington, we support any change to the state's fluoridation rules, including the petition before you today that recommends against fluoridation chemicals to be put in our drinking water. I think the petition before you today is not as strong as it should be. I think the recent study released by the National Toxicology Program is strong enough to warrant a cease and desist of adding fluoride chemicals into water supplies.
Ingesting fluoride is no way to target a fluoride treatment that can be applied to the teeth – IF fluoride is determined to be beneficial to the health of our teeth. Again, I would support, to a great extent, a forum, an actual working group review of fluoridation.
Two public commenters spoke in opposition to Bill’s petition. The first commenter said that the public needs to continue discussing the well-managed, appropriate levels of fluoridation in our water, but not to take the fluoride out. “Those levels that we have that are safe and low enough to prevent cavities and strengthen teeth,” she said. “The bottom line is what makes us smile. The benefits of fluoridation and safe optimal levels cost only 38 cents per person per year, and we know that the financial pain and suffering of children, parental time off of missed school is too great a risk to take.”
The other opponent to Bill’s petition was a policy analyst with the Washington State Medical Association. “Healthcare providers support fluoridation to prevent and reduce tooth decay, cavities, and other oral health risks,” she said. “Definite evidence supports the fluoridation of water to prevent tooth decay. and we urge opposition to this potential rulemaking.”
Two other public comments were in support of newborn screening, and three public comments revealed more about the COVID-19 debacle that the board has refused to address.
ICWA Director Lisa Templeton informed the board about a research paper that was published on October 15 that called out the Washington Department of Health (DOH) for significant data quality issues and showing that DOH data should not have been used to guide policies during the pandemic.
Lisa then said the following:
The article, Evaluating Data Integrity and Reporting Challenges in Public Health: Lessons from COVID-19 Data Collection in Washington State, was written by Clifford Knopik, a computer scientist specializing in data and analysis. He approached the Institute of Pure and Applied Knowledge (IPAK) to get the word out. The article was peer-reviewed and published in the journal Science, Public Health Policy and the Law.
Summarizing the paper, Mr. Knopik said that the “Washington State Department of Health's (WA DOH) COVID-19 data had significant errors, rendering it unreliable for use in decision-making and visualizations.”
Six types of data errors were found that undermined the entire dataset's credibility:
Five different types of data were misclassified as the "Symptom Onset Date," which misled both Governor Inslee and the public in evaluating the pandemic's status.
This misclassification caused inaccurate representations of COVID-19 cases, hospitalizations, and deaths.
Probable COVID cases were incorrectly classified as confirmed cases, further distorting the charts and graphs.
WA DOH labs used PCR tests at cycle thresholds that were high enough to potentially produce false positive results.
Unknown data was included in WA DOH's charts:
97% of unknown cases came from labs outside WA DOH's oversight, making it impossible to verify whether the tests were accurate, false positives, or duplicates.
50% of the Symptom Onset Date information displayed in charts was missing, with the remaining half filled by incorrect date classifications.
In comparisons of vaccinated vs. unvaccinated individuals, the data for the unvaccinated was skewed higher because WA DOH included months before vaccines were widely available (February to mid-April 2021).
The paper provides citations and examples to demonstrate that:
At least 97% of the COVID data collected by WA DOH was unreliable and unfit to be used for graphs, and to inform the public and decision makers.
The errors skewed in the direction to make cases appear worse and to make unvaccinated numbers appear worse.
This paper helps explain why Washington was different from other states, consistently promoting data that favored DOH policies and claims, especially now that it has been widely acknowledged that the vaccine never worked as promised, and that restrictive measures were ineffective. Israel is one such country where the admission came in 2022. This quote from Ehud Qimron, a leading Israeli immunologist, sums up their country’s outcome and should make everyone question any of the Washington DOH claims:
Two years later, you finally realize that a respiratory virus cannot be defeated and that any such attempt is doomed to fail. You do not admit it, because you have admitted almost no mistake in the last two years, but in retrospect, it is clear that you have failed miserably in almost all of your actions, and even the media is already having a hard time covering your shame.
Be Brave Washington leader Natalie Chavez commented on the injustices of the COVID-19 shots:
A lot has happened since the last meeting that I attended in regard to COVID vaccine-related lawsuits with positive outcomes including some with multi-million dollar rewards to plaintiffs who were terminated for not willing to get experimental COVID-19 vaccines injected into their bodies. Injections that we know do not stop infection and do not prevent transmission. Injections that did not undergo eight to ten years of safety testing and had no long-term clinical trials in animals or humans. Injections that we know have caused harm, even death, to numerous individuals, including many Washingtonians, which include members in my own community.
You can learn more about the COVID vaccine-injured at the website React19.org.
COVID vaccine-injured individuals in the Netherlands filed a lawsuit against Bill Gates, Pfizer CEO Albert Bourla, and the Dutch state.
Judge Rules Bill Gates Must Face Vaccine-Injured in Netherlands Court • Children's Health Defense
Last month, the District Court of Leeuwarden found sufficient evidence that the claims against Bill Gates and other Defendants are connected and based on the same complex of facts. The next Court hearing is scheduled for this month November 27th.
One of the COVID vaccine-injured plaintiffs has since died, and another one is so severely vax-injured that she can no longer speak, so her father spoke on her behalf at a Court hearing in Netherlands on September 18th.
I also want to bring to your attention to the Southwest District Health Board in Idaho, which oversees six counties in Southwest Idaho. Last month on October 22nd, they became the first local health department in the United States to remove experimental COVID-19 injections from its taxpayer-funded sites, thirty healthcare sites.
That health board voted to remove the vaccines after approximately 300 of their community members made public comments urging the health board to stop promoting COVID-19 injections.
One Idaho nurse said that she knows many people who have been injured by the COVID-19 vaccines. And a physician said, "The people of this District were demanding answers. Many came forward with heart-breaking stories of vaccine injury."
The COVID cards are definitely collapsing, along with the COVID narrative hat was propagated by the FDA, CDC, on social media, the mainstream news, and in our state at every level from the Department of Health to local health departments.
I started my public comment by apologizing to the board for again “bringing up the injuries from the COVID-19 shots here in our state but that someone had to do it, and you people on the board are not doing it.”
Stating my case:
You refuse to acknowledge this as an issue, such as when Scott Lindquist said at the meeting last April that it’s only throwing up a number of 200 injuries as if it’s no big deal. But that number is actually for the number of deaths—238 to be exact. The real number for injuries is 24,111 reports here in Washington to VAERS after the COVID shots. That’s a lot of coincidences, especially for the 3,482 cases of onsets that began within one day following the COVID-19 shot.
These are not just sore arms, either.
139 seizures in Washington; 24 of them in the first 24 hours onset. That’s a lot of coincidences. And do you call this one a coincidence:
VAERS ID: 1490529
25-year-old female with no history of seizures. A week after the first COVID shots, she had a seizure, and then a week after her the second dose she had another seizure while driving and crashed her car into a ditch.
34 cardiac arrests, in which 5 occurred within one day, and that’s not including the 69-year-old listed under road traffic accidents who had just received his first Moderna shot and was pulling into the observation area when he lost, conscious and control of his truck and crashed it into a light pole.
VAERS ID: 1017743
But at least have you ever apologized to the people of Washington for the 102 cases of Bell’s Palsy following the jabs in which the onset of ten of them occurred within one day. No, you just carry on as if nothing has happened. Or how about the 23 cases of Guillian-Barre Syndrome?
including a nine-month-old? Did you ever apologize to the people of Washington for that? Or how about the 136 cases of myocarditis reported to VAERS following the COVID-19 shots here in Washington in which 23 of those onsets began within one day after taking the shot.
Or how about the 119 reports of irregular menstrual bleeding; I saw over a dozen cases of much heavier than normal bleeding and over ten cases of menstrual bleeding within 24 hours for those on birth control, and two cases of bleeding for postmenopausal women.
Or how about the 50 listed as Spontaneous abortions here in Washington, and these are not listed as deaths in VAERS; Yes I know the DOH website says that miscarriages occur in 10-20 percent of pregnancies, but I counted at least a dozen spontaneous abortions that occurred within three days of taking the COVID-19 shots.
As soon as I returned to my seat, Bill Osmunson turned to me and said, “I got pericarditis from the COVID-19 shot.” Later on, he told me that he took the second Moderna shot on January 15, 2021, at the Harbor View medical center for one reason only: To allow him to keep treating his dental patients. When he initially reported his case to VAERS, he misspelled the doctor’s name who diagnosed his pericarditis at the Overlake Medical Center in Bellevue, so the CDC called him up to correct this. Pericarditis is the swelling and irritation of the thin, saclike tissue surrounding the heart, and Bill is one of 105 VAERS entries for pericarditis in Washington.

The VAERS report that most likely fits Bill’s adverse event, with no preexisting conditions, has the following submitted write-up:
VAERS ID: 1396408
Diagnosed with pericarditis. I have slowly gotten more tired until I had significant aches, upper chest pain near sternum, intercostal muscles SCM and scalene very sore, couldn’t breathe deep and hard to walk up steps. Couldn’t sleep and pain radiating down left arm. Went to ER 1 AM and they did EKG, flood work and chest X-ray. All vitals normal. Sent me home because I was feeling better having sat up. Two nights later significant pain, about 6 out of 10, couldn’t sleep, couldn’t breathe fully, went back to ER. More tests and diagnosed with pericarditis.
Bill told me that it took him three years to get his energy back. He then told me about incidents he had witnessed concerning vaccines. One student of his couldn’t stop limping, and he told Bill that it was “a reaction from the live Polio virus vaccine.” He told me that a school superintendent in Bonney Lake, where Bill lived at the time, shut down three elementary schools due to pertussis; the 113 children who went on to get pertussis had all received the pertussis vaccine. All those who did not get the vaccine, Bill said, did not get pertussis. Bill at one time mentioned a Cochrane Study to the Sophie Trettevick Health Center in Neah Bay about the ineffectiveness of the flu shot, but they said, “That’s just one study.” They went on to give the flu shot to seventy-six of their seventy-seven patients.” Bill said he would speak out against vaccines at the Board of Health meetings, but he’s been too focused on the hazards of water fluoridation.
For the Local Health Jurisdiction Health Update at 10:25 a.m., Jennifer Freiheit, who is the interim director of Thurston County Public Health and Social Services, said that social loneliness and isolation is the number one public health crisis in the county. She would be holding a virtual summit and then a social media campaign to combat this. Board Member Tao Kwan-Gett then told Freiheit that he, too, understood this issue, and that’s why the DOH had started a Be Well Washington program in which the fourth pillar is about the importance of social connections that “can occur with neighbors, family, friends, coworkers, and other people in our community.”
The ICWA Weekly News 11-6-24 covered the Be Well Washington initiative.
I immediately thought that if social connection was so important, then why did the Washington government enforce lockdowns and other untested restrictions during the COVID-19 panic, notably forcing the elderly to die in hospitals and nursing homes without having their families by their sides? Then when the shot rollout occurred, why did Tony Fauci and other government officials instruct people to exclude family and friends from social gatherings, family events, holidays, and even funerals based on whether or not they received the jabs? Naturally, none of this was mentioned.
Just as I was thinking about how much the hypocrisy of the DOH never ceases to amaze me, four panel members from the Department of Health and two panel members from the Department of Ecology sat at the speaker’s table and gave their “State Agency Response to Per- and Polyfluoroalkyl Substances (PFAS).” For one-and-a-half hours, each speaker spoke at length about the hazards of this toxic substance and ways that they could combat it by way of more public outreach. Claire Nitsche from the DOH had even contracted with a social marketing research firm C+C and their ‘workbook.’

This led me to wonder whether this was the same research firm that the DOH used when it wrote the following in its $35 million proposal to the legislature to restore trust in public health by combatting misinformation: “DOH saw firsthand the impact of these disinformation campaigns through audience research, ongoing polls, and community feedback. As a result, some people have become more likely to believe something false from a friend or family member than something true from the government, which in some cases, leads to decisions not to access life-saving public health services.”
But screaming in my head on top of all that was that if the DOH was going to put all this time and effort into researching and promoting the health hazards of PFAS, why haven’t they been doing the same thing with the toxic spike protein in the COVID-19 mRNA gene therapy shots?
Bill Osmunson was thinking along the same lines about water fluoridation. He wrote the following to Washington State Representative Bill Ramos:
About an hour was spent on PFAS. Six people from the Department gave presentations on the potential for harm from probably more than six areas of the state with high concentrations. Foods, fish, chicken, beef, pans, lubricants, fake lawns, and so much more of possible concern. They may be asking for funding and a whole new team of experts to work on the potential problem and how to reduce the risk. OK, I agree. PFAS is a concern, and the solution is complex but does it deserve six people and an entire new bureaucracy when much of the problem so far centers on military, airports and firefighting training and of course education and reducing population exposures? With an unlimited taxpayer budget, go for it. . . . However, PFAS is not my area of expertise.
Compare those two valid concerns with fluoridation.
#1. The Board will not let me give a presentation. Max, 3 minutes, no questions, no response, but the Department gets much more time to extol the miracle benefits . . . And the law says to assure safe and says nothing about weighing any benefit.
#2. The law says the Board of Health shall provide a forum. . . . However, 3 minutes or 2 minutes is not a forum.
The Board of Health put on this PFAS show because they received orders from their “bosses” at the federal level to do so. Page 117 in the meeting packet, dated November 13, 2024, from Board Member Kate Dean says as much:
On June 12, 2024, in response to the Environmental Protection Agency’s adoption of a maximum contaminant level (MCL) for Per- and Polyfluoroalkyl Substances (PFAS), the State Board of Health (Board) initiated three rulemakings to revise the Board’s PFAS requirements for drinking water. With this action and prior rulemakings related to PFAS, the Board joins many state agencies working in different capacities to research and mitigate these contaminants.
As for Bill’s petition, Dean wrote on page 196 in the meeting packet:
Background and Summary: The Administrative Procedure Act (RCW 34.05.330) allows any person to petition a state agency for the adoption, amendment, or repeal of any rule. Upon receipt of a petition, the agency has sixty days to either (1) deny the petition in writing, stating the reasons and, as appropriate, offer other means for addressing the concerns raised by the petitioner, or (2) accept the petition and initiate rulemaking.
On October 3, 2024, the State Board of Health (Board) received a petition from Washington Action for Safe Water and Bill Osmunson, DDS MPH. The petitioners request the Board consider amending WAC 246-290-220, Drinking Water Materials and Additives, within the Group A Public Water Supplies rules.
The Board has the authority under RCW 43.20.050 to adopt rules for Group A public water systems as defined in RCW 70A.125.010. Chapter 246-290 WAC establishes the standards for these water systems related to their design, construction, sampling, management, maintenance, and operation practices. The purpose of these rules is to define basic regulatory requirements and to protect the health of consumers using public drinking water supplies.
The petitioners request that The Board amend WAC 246-290-220 to include a new subsection related to water fluoridation that states either of the following:
• The Board of Health does not recommend adding fluoridation chemicals to water with the intent to treat humans or animals; or
• In keeping with the Federal Safe Drinking Water Standards, the Board of Health does not recommend chemicals, including fluoride compounds, be added to the water with the intent to treat or prevent disease in humans or animals.
The petitioner included attachments to support the request, located in the Board materials. Shay Bauman, Board Staff, will present the Board Members with information related to the petition and recommendations.
Bill Osmunson’s attachments to support his request are on pages 27 through 85, and again on pages 92 through 94 in the meeting materials packet.
But instead of the six “panel of experts” used for the PFAS discussion, only Board Staff Member Shay Bauman gave a presentation.
The first point raised for declining Bill’s petition came with the following slide in which Bauman read the boldfaced bullet point as well as reading the bottom of the slide that this subsection is not relevant to fluoride.
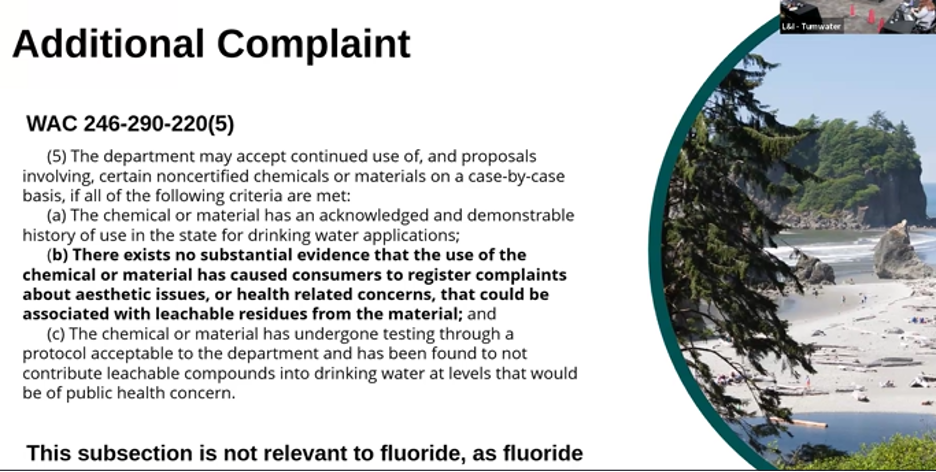
“With this item, the petitioners state that they are again registering a complaint that dental fluorosis causes aesthetic and functional harm and other related concerns citing this section of the WAC,” she said. “A reminder to the board members that this part of the rule subsection 5 is not relevant to fluoride as fluoride is required to be certified under Standard 60. As I discussed in that last slide.”
She then put up the next slide about the National Toxicology Program (NTP) and said the following:

I wanted to highlight the monograph on the state of science concerning fluoride exposure and neurodevelopment and cognition conducted by the National Toxicology Program or NTP within the Department of Health and Human Services. I'll refer to this study as the NTP Monograph or monograph. The NTP conducted a systematic review of published literature on the association between fluoride exposure and neurodevelopment and cognition. Its findings were published in August of this year. Among its key findings is moderate confidence that high levels of fluoride exposure, such as drinking water that contains more than 1.5 milligrams per liter of fluoride are associated statistically with lower IQ. In children there are some important considerations with the findings. The study evaluates total fluoride exposure and emphasizes that its findings do not show the health effects of drinking fluoridated water alone. Similarly, it does not find harm associated with the current recommended levels for optimally fluoridated water. The level for optimal fluoridation is 0.7 milligrams per liter. Establish in WAC 24629460 and in line with the national standards.
At this point, Bill Osmunson, by now seated right next to me, growled, “This is bullshit.”
Later on, Bill told me that to say 0.7 milligram per liter is safe would require several assumptions.
No other sources of fluoride are ingested.
Everyone drinks the same amount of water at one liter per day.
Everyone has the same degree of health. Mean health.
No margin of safety is needed or provided.
The US District Court reporting fluoridation as a reasonable risk is ignored.
No one infests other synergistic oxidants.
Bauman went on to say the following:
This is less than half the level studied in the monograph. The study notes that many substances are healthy and beneficial when taken in small doses but may cause harm at higher doses. And specifically that more research is needed to better understand if there are health risks associated with lower fluoride exposures mentioned in our last meeting. The board is coordinating with the Department of Health to review the study and its findings and I know that the petitioner has been invited to participate in that review as Designee Tao Kwan-Gett mentioned at our last meeting in October.
The next slide was of a district court ruling in California:

Bauman went on to say, “The ruling doesn't require the EPA to ban water fluoridation, nor does it specify what action they must take. The EPA can conduct rulemaking to consider options or appeal the decision in addition to reviewing the monograph. As I mentioned, we are monitoring what the EPA will do as a result of this ruling. There's obviously a lot happening right now that we're monitoring, and evidence still supports that the optimal fluoridation level of 0.7 milligrams per liter is safe.
Bauman then showed the final slide, which recommends a declining of Bill’s petition.

She said the following:
Fluoridation is not currently mandated in the rule. In addition, the alternative wording is particularly problematic because it implies that there may be no additives to drinking water.
This includes things like chlorine, which protects against a number of waterborne illnesses, such as cholera, typhoid fever, hepatitis A and Giardia. It would be especially dangerous to public health. For these reasons my recommendation is to decline the petition for rulemaking and with that I'm available for questions.
Patty Hayes said, “Alright. So, let's open this up for questions from the board.” Naturally, since Bill was not on the board, he was not allowed to ask any questions or raise any issues with Bauman’s recommendation.
All eyes eventually turned to DOH Chief Medical Officer Tao Kwan-Gett, who was asked, “Will there be a report back to the board on that review that's happening with partners in the Department of Health? Or could you give us any other update on that?”
Gett replied, “I'm sorry. I don't know what the timeline for that is.” He added that Assistant Secretary for Environmental Public Health Lauren Jenks is the lead for this along with Michele Roberts. “So, they would be the ones who would be more knowledgeable about this,” he said.
With one board meeting a month, and fluoridation a main agenda item, you’d think the Chief Science Officer could have brought a little more info to the meeting!
After discussion about the uncertainty of a timeline from the EPA, Kate Dean said,
Given the unknown timeline, and next steps of the EPA. I would be disinclined to support this petition, knowing that we will be potentially presented with additional information or confirmation of information that supports our current rule. So, I am inclined to deny the petition. I'm happy to make a motion if that would be helpful.
After Dean made the motion to deny the petition, Tao Kwan-Gett seconded it. During the ensuing discussion period, the consensus among the board was to wait for the scientific review as well as fully understanding the board’s role of not making recommendations. Socia Love said, “With regard to the fact that the rules don't mandate water fluoridation but provide guidelines if a jurisdiction chooses to fluoridate.”
I then clearly heard Bill Osmunson growl, “That doesn’t protect the public.”
Board Member Michele Davis then made the following clarifications:
The problem is that the placement of a recommendation within a rule, when rules are standards, and this is focused on drinking water systems. And it's the drinking water systems that have to comply with the standard. That's where the disconnect is. the Board can make recommendations to the governor, to the secretary, to the legislature, but we don't use rulemaking as the mechanism for making recommendations. So, I just wanted to provide that clarification for the discussion.
After Socia Love and others thanked Michelle Davis for that clarification, the board voted unanimously to deny Bill’s petition.
Bill jumped to his feet and said aside to me, “Before I scream at them, I’m going to walk out. It’s all a bunch of bullshit,” as he stormed out of the room.
(The ICWA team understands Bill Osmunson’s frustration since he has been advocating tirelessly for many years and warning the DOH/BOH about the unnecessary risk of drinking water fluoridation. But we’re also excited that this experienced dentist will likely be invited to the technical advisory group on water fluoridation).
More Debunking of the Claim That One Is More Likely to Get Myocarditis from COVID-19 Than from the Shots
As most of our readers would expect, given how ineffective the COVID jabs have been, the damage from taking the shots is much worse than reported by the Washington Department of Health.
Last July, ICWA Weekly News ran a story debunking Dr. Anita Chopra’s claim that “Studies have found that unvaccinated patients with COVID-19 were 16 times more likely to develop myocarditis than patients without COVID-19.”
Dr. Chopra referenced the research article published in August of 2022 in the journal Circulation titled: Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex.
This study, a probably attempt to support the failing medical intervention, drew the following conclusion:
Overall, the risk of myocarditis is greater after SARS-CoV-2 infection than after COVID-19 vaccination and remains modest after sequential doses including a booster dose of BNT162b2 mRNA vaccine. However, the risk of myocarditis after vaccination is higher in younger men, particularly after a second dose of the mRNA-1273 vaccine.
Now, this past week, Epidemiologist Nicolas Hulscher with the McCullough Foundation team of scientists and doctors has exposed much more serious cardiac event data in King County where the opposite was true.
Peer-Reviewed Study Reveals 1,236% Surge in Excess Cardiac Arrest Deaths Among 2 Million COVID-19 Vaccinated Individuals [Video; 21 mins]
In the video accompanying his post, Dr. Hulscher made the following statement:
What we found was among 98 percent of the King County population that is vaccinated, received at least one dose, there was a 1,200 percent increase in excess cardiac arrest deaths, 25 percent increase overall in total cardiac arrests. So, the survival rate dropped of EMS attending these cardiac arrests, and cases of obvious death increased dramatically since the vaccines rolled out. So, all this cardiac arrest among a sample size of two million people in this county, we found that it takes about two million people to detect this sort of safety signal. These findings are a very strong safety signal that must be considered by regulatory authorities to prevent cardiac arrests from happening.
Dr. Hulscher’s article published in the Journal of Emergency Medicine published October 24 provided the following results:
Approximately 98% of the King County population received at least one dose of a COVID-19 vaccine by 2023. As of August 2nd, 2024, there have been approximately 589,247 confirmed COVID-19 cases in King County. In 2021- 2022, Total EMS attendances in King County sharply increased by 35.34% from 2020 and by 11% from pre-pandemic years. Cases of 'obvious death' upon EMS arrival increased by 19.89% in 2020, 36.57% in 2021, and 53.80% in 2022 compared to the 2017-2019 average. We found a 25.7% increase in total cardiopulmonary arrests and a 25.4% increase in cardiopulmonary arrest mortality from 2020 to 2023 in King County, WA. Excess fatal cardiopulmonary arrests were estimated to have increased by 1,236% from 2020 to 2023, rising from 11 excess deaths (95% CI: -12, 34) in 2020 to 147 excess deaths (95% CI: 123, 170) in 2023. A quadratic increase in excess cardiopulmonary arrest mortality was observed with higher COVID-19 vaccination rates. The general population of King County sharply declined by 0.94% (21,300) in 2021, deviating from the expected population size. Applying our model from these data to the entire United States yielded 49,240 excess fatal cardiopulmonary arrests from 2021-2023.

And they concluded the paper with:
We identified a significant ecological and temporal association between excess fatal cardiopulmonary arrests and the COVID-19 vaccination campaign. The increase in excess cardiopulmonary arrest deaths may also be attributed to COVID-19 infection and disruptions in emergency care during the pandemic. Urgent further research is needed to confirm our observations with attention to risk mitigation for incident events and improved survival with resuscitation.
Furthermore, this past Monday, November 18, Dr. Nicolas Hulscher posted that identified flaws in another study, this time published in JAMA on August 26, 2024, by Semenzato et al claiming that patients who develop myocarditis following an mRNA COVID-19 vaccination experience fewer cardiovascular complications at 18 months compared to those with alleged myocarditis following a COVID-19 infection.
Dr. Hulscher debunked the study in the following manner:
We identified major methodological flaws in their study that led to significantly biased conclusions. Thus, we (Nicolas Hulscher, MPH, Jessica Rose, PhD, and Peter McCullough, MD, MPH) submitted a Letter to the Editor to JAMA to highlight these concerns.
Unfortunately, they declined to publish our research letter “because of the many submissions we receive and our space limitations in the Letters section.” We were fortunately able to publish our concerns in the non-partisan journal Science, Public Health Policy, and the Law: Letter to the Editor: Long-Term Prognosis of Patients with Myocarditis Attributed to COVID-19 mRNA Vaccination, SARS-CoV-2 Infection, or Conventional Etiologies:
In conclusion, the study by Semenzato et al. is misleading. SARS-CoV-2 infection does not cause serious myocarditis [7, 10], whereas COVID-19 vaccination is well recognized to cause symptomatic and fatal myocarditis [6, 11]. Future prospective cohort studies should classify patients correctly, have extended and equal windows of observation, and clinical adjudication with exam, ECG, blood biomarkers, and cardiac imaging. The use of automated data sources alone should not be relied upon for comparative studies because it is subject to investigator bias and is greatly misleading.
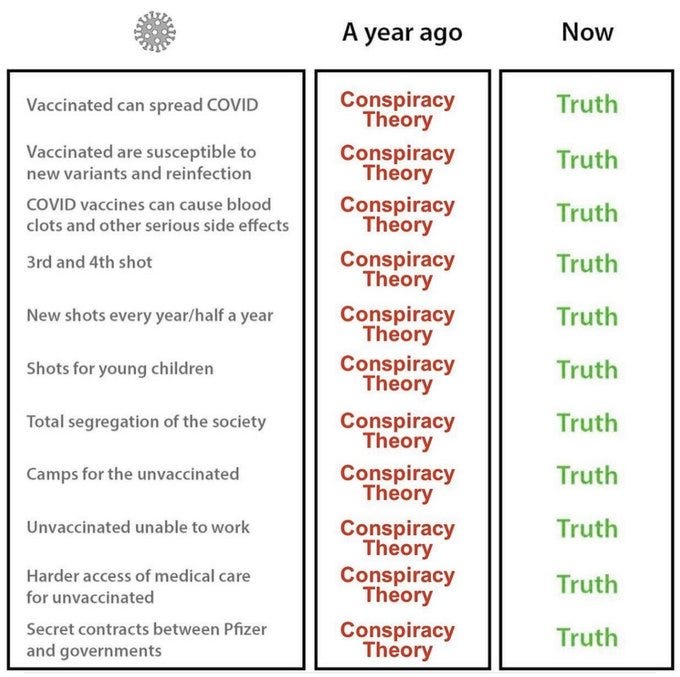
Thank you from Patrick.net on substack, some memes of truth
Aaron Siri speaking truth on X:
Something RFK Jr. will be working on:


Thank you for all of this information and for everything you do.