


ICWA Weekly News 7-16-25
Saturday parade in Covington; Moderna Spikevax approved, even with history of adverse events, Marketing vaccines to rural Washington communities; July 28 lunchtime event in Spokane.


In this issue:
Saturday Parade in Covington
Moderna Spikevax Approved Even With History of Adverse Events
Marketing Vaccines to Rural Washington Communities
Other events and memes
July 11 episode of Informed Life Radio – notes and links
WA State: Concerning Public Health Policy Shifts
(Replay Links: Informed Life Radio website, ICWA on X, Facebook, Rumble, CHD.TV)
Hosts discuss WA State Attorney General’s latest Domestic Extremism Task Force meeting, where extremism is framed as a “public health” problem. Hosts also discuss the recent Department of Health (DOH) Vaccine Advisory Committee (VAC) meeting, which was the first since DOH announced it would follow the VAC's Covid shot recommendations, rather than the new CDC's.
Domestic Extremism and Mass Violence Task Force | Washington State
The next Task Force meeting is September 12, 2025
Vaccine Advisory Committee (VAC) | Washington State Department of Health
On Saturday, July 19, Join ICWA and CHD WA Members at the Covington Days Parade
Saturday, Saturday, Saturday - ICWA and CHD members will march in the Covington Days parade.
Please RSVP to lisa@informedchoicewa.org, or if you have questions.
ICWA’s South Puget Sound team will meet at 9:00 AM for a 10:00 AM start. Walking should finish up by 11:00 or 11:30 AM, depending on the start order. Again, connect with Lisa to get the finer details.
Volunteer gifts are still available - water bottle or tote.
Fun is guaranteed.
Moderna Spikevax Approved Even With History of Adverse Events
Last Thursday, July 10, STAT News reported on the FDA’s shift from emergency use authorization to approval for Moderna’s COVID-19 shots for the ages six months to eleven years:
Moderna’s Covid-19 vaccine for children has been given full Food and Drug Administration approval, making it the first Covid vaccine for kids in the United States that will no longer be administered under an emergency use authorization.
But the approval comes with a proviso: It is for use in children who have at least one medical condition that puts them at increased risk of severe illness from Covid, according to the FDA.
Dr. Peter McCullough was interviewed by Lindell TV news and he wrote the following in his Focal Points publication about this proviso:
Restricting vaccination to children with baseline medical problems such as congenital heart or lung disease could make the shots even more risky because a side effect such as myocarditis or blood clots could be fatal in children who are already compromised.
Conservative Ladies of America pointed to these risks and others from the Spikevax package insert:
Parents deserve full transparency. The safety section of the Spikevax insert reads like a list of red flags:
Myocarditis and pericarditis are noted as known risks, especially in young males.
Reported symptoms in children include fainting, seizures, vomiting, irritability, and even poor feeding in infants.
The insert even admits: “vaccination may not protect all people who receive it.”
As for the actual injuries, Conservative Ladies of America said this:
Let’s not forget: This is the same product that was rushed into use under “emergency” status, with shielded liability and limited transparency. Now, years later, we’re expected to just trust that everything checks out? Trust the same FDA that rubber-stamped this approval while vaccine injuries remain underreported and underacknowledged?
Keeping in mind underreporting, VAERS shows 4,834 adverse events following the Moderna COVID-19 shot for the six-month to eleven-year-old age group in the United States and its territories. Just for comparison’s sake, there were 19,068 adverse events after Pfizer/BioNtech shots in that age group.
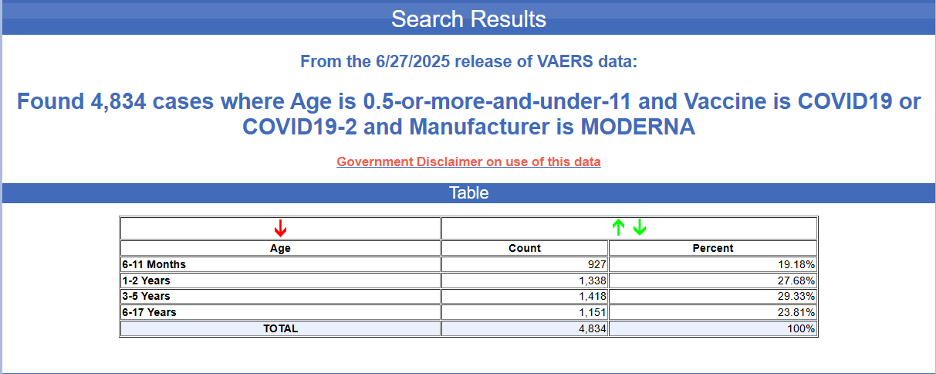
As for the 6 months to 11 years old age group in Washington, VAERS shows 309 cases of adverse events following any COVID-19 shot, including sixty-one reports for the six-month to one-year-old group following the Moderna COVID-19 shot.
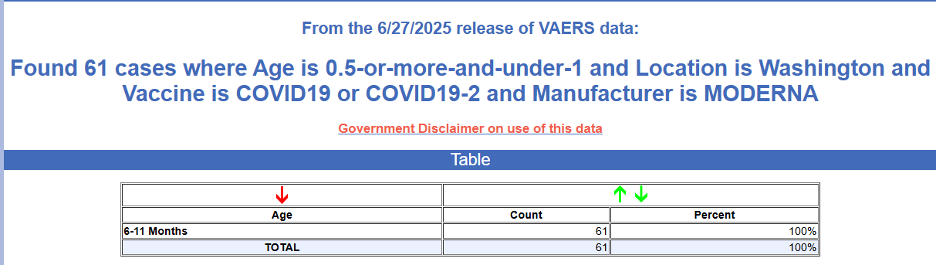
The latest report for this under-1-year-old group was from December 12, 2024.
Keeping in mind that medical error is the third leading cause of death in the U.S, as we reminded readers in the June 4, 2025 issue of ICWA Weekly News, this report was about a medical error.
VAERS ID: 2815713. Submitted write-up: A 10 month old was given an extra dose of a Moderna vaccine. Her first Moderna vaccine was on 10/8/24, second dose 11/25/24 and the extra dose was given on 12/9/24. This error happened because the beyond use date was written down incorrectly on the vaccine that was given on 11/25/24. The clinic thought that the dose on 11/25/24 was expired so they had the patient come in for the repeat dose on 12/9/24. We then discovered that the vaccine given on 11/25/24 was potentially not expired. We are unable to 100% verify if it was expired because it is all hearsay. I already contacted Moderna and they directed me to the CDC Interim Clinical Considerations for Use of COVID-19 Vaccines: Appendices, References, and Previous Updates. If a higher than authorized dose is administered, the CDCs recommendation is to not repeat a dose. I also contacted the DOH nurses and they said "First, thank you for contacting us with your question about Moderna. Based on the information you provided in you email, you are right on track. There have been reports of patients receiving higher-than-authorized doses in the past, with no major side effects reported although the child may experience more pronounced side effects (like a soreness at the injections, site, etc.) Below is a link to a study on individuals that received extra doses of vaccine it was before COVID, but has good information on what could happen based on other vaccines: Is there any harm in administering extra-doses of vaccine to a person? Excess doses of vaccine reported to the Vaccine Adverse Event Reporting System (VAERS), 2007-2017 - Please be sure the incident is reported in VAERS - Report an Adverse Event as well. This is the tool they used for the study above. It is helpful for CDC to have this information so they can keep track of potential trends that may develop and respond, if needed.
Continuing to break down Washington adverse event data into age bands, there have been 101 adverse events for the one through three-year-old range following the Moderna COVID-19 shot.
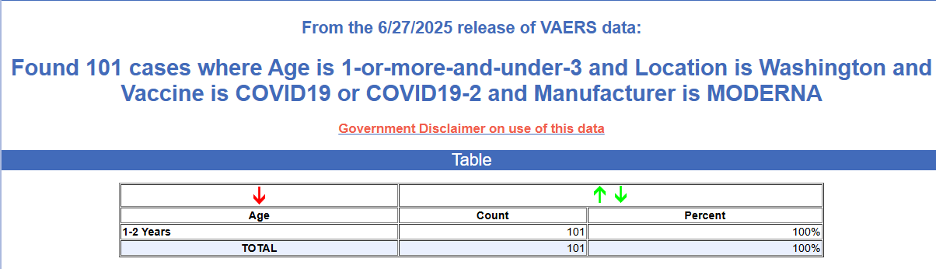
One of those 101 cases here in Washington resulted in the death last October of a male who was a little less than two years old.
VAERS ID: 2798693
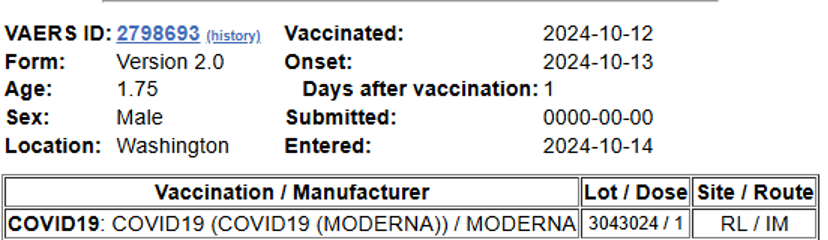
The submission says that the boy died one day after receiving the Moderna shot on October 12, 2025. The above snapshot shows that the boy received just the COVID-19 shot. The submission lists no preexisting conditions or current illnesses. The submitted write-up simply says, “Death.”
Washington has had 105 reported events for the three through six-year-old age range following the Moderna COVID-19 shot.
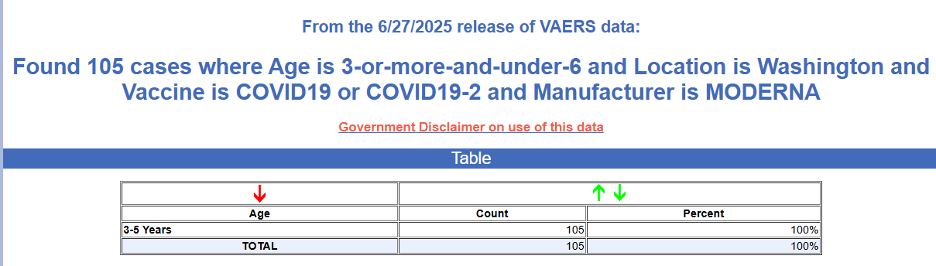
The latest event reported was from April for a COVID-19 shot delivered to a four-year-old female.
VAERS ID: 2837983. The child was also administered a MMR and Hepatitis A shot. Here is the submitted write-up: Child had coughing, redness of injection site followed by itching and erythroderma of face, trunk, less on extremities with some nausea and fatigue within 5 minutes of vaccination. Coughing resolved spontaneously. No wheezing on exam. Benadryl 12.5mg given and epinephrine .015 mg given with improvement of skin redness and itching. Child previously received MMR and Varivax separately without reaction. Vaccine was given in conjunction with first dose of Hepatitis A and COVID.
The reported case before that was another of medical error.
VAERS ID: 2818575. The three-year-old female received just the COVID-19 shot last September.
The submitted write-up shows this error: Patient was given extra doses of COVID and Influenza vaccines. Received Covid and Influenza on 12/10/2024. Patient was observed 15 minutes post vaccination once error was discovered, and she had no adverse reaction at that time.
Washington has had forty-two reported adverse events for the six through eleven-year-old range following the Moderna COVID-19 shot.
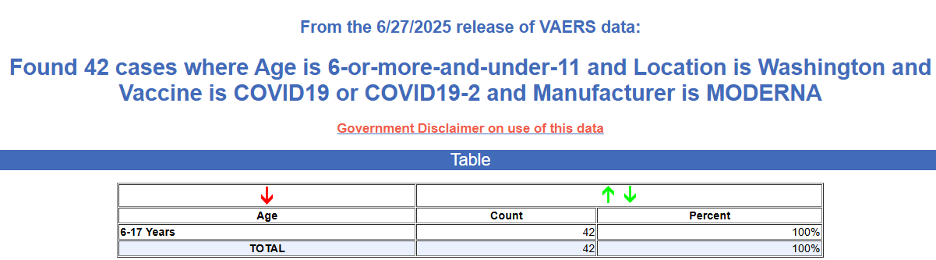
The above listing under “Age” column reads “6-17” years, but a look at each entry shows that the ages for all the reports are from six through eleven as the filter criteria are correctly set. If the full 6-17 year age range was queried, it would show 457 adverse event reports, but we constrained our search to match the Spikevax approval at capped at 11 year olds for better comparison.
Both of the reports for 2025 for the six through eleven age range were again of medical error. Here they are:
VAERS ID: 2835592. Submitted write-up for this ten-year-old female: Patient is only 10 years old and was given the higher dose (12+ year) vaccination.
VAERS ID: 2846964. Submitted write-up for this six-year-old male: Patient received an expired dose of Moderna COVID vaccine for ages 6 months-11 years. Expiration date was 6/21/25 but medical assistant misread this as 6/27/25 and thus administered the dose on 6/23/25 after it was already expired. Barcode scanning technology was used AFTER administration and so the error was not caught until post-administration. No harm occurred to patient.
With this approval of SpikeVax, ICWA members are wondering when all the other emergency-use-authorized products for COVID-19 should now be taken off the market.
Marketing Vaccines to Rural Washington Communities
On September 25, 2023, the CDC issued a marketing strategies special report titled Vaccination in Rural America as part of a State of Vaccine Confidence SoVC) series. The report is now located in an archived area of the CDC website.
A look at vaccine uptake in the rural counties of Washington shows why the CDC desired to issue such a report.
We take a look at the administration of the COVID-19 shots in Washington’s rural counties using some of the immunization coverage information presented by Jamilia Sherls of the DOH to the BOH in May of 2023. You can see similar maps with more current data at Immunization Measures by County Dashboard | Washington State Department of Health, the COVID-19 Dashboard, and other explanatory data on the DOH website.
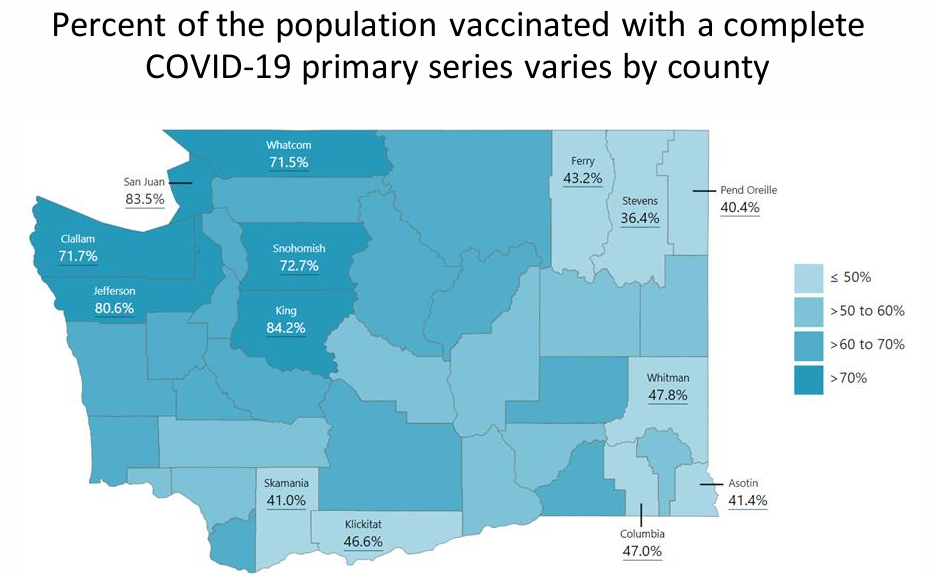
The following look at eight of the seventeen least populated counties in Washington show why the CDC would like to promote a marketing campaign for rural Washington:
Stevens ranks 22nd most populated and has just 36.4 percent receiving the COVID-19 shots.
Whitman ranks 23rd most populated and has just 47.8 percent receiving the COVID-19 shots.
Klickitat ranks 29th most populated and has just 46.6 percent receiving the COVID-19 shots.
Asotin ranks 30th most populated and has just 41.4 percent receiving the COVID-19 shots.
Pend Oreille ranks 33rd most populated and has just 40.4 percent receiving the COVID-19 shots.
Skamania ranks 34th most populated and has just 41 percent receiving the COVID-19 shots.
Ferry ranks 36th most populated and has just 43.2 percent receiving the COVID-19 shots.
Columbia ranks 38th most populated and has just 47 percent receiving the COVID-19 shots.
As for the childhood immunization series schedule, the following map for 19–35-month-olds could also explain the CDC’s desire for vaccine marketing to target to rural Washingtonians.
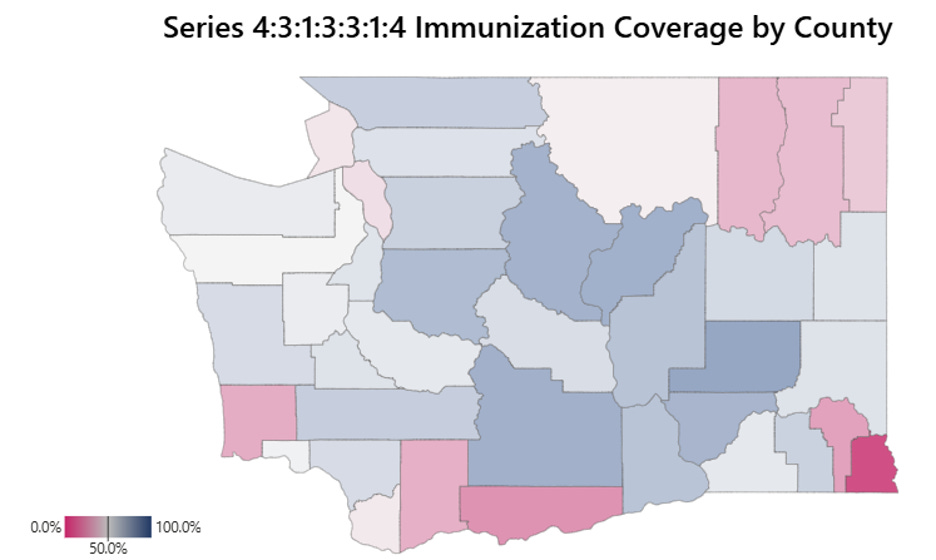
The Series 4:3:1:3:3:1:4 reflects the number of shots received to be considered up to date - four DTaP, three polio, one MMR, three Hep B, three Hib, one Varicella, and four pneumococcal (PCV) for a total of nineteen injections by the age of 35 months.
Note the low uptake in eight of the seventeen least populated counties in Washington:
Stevens is ranked 22nd in most population and has just 36.7 percent receiving the immunization series.
Pacific is ranked 28th in most population and has just 32.8 percent receiving the immunization series.
Klickitat is ranked 29th in most population and has just 26.6 percent receiving the immunization series.
Asotin is ranked 30th in most population and has just 10.7 percent receiving the immunization series.
Pend Oreille is ranked 33rd in most population and has just 39.6 percent receiving the immunization series.
Skamania is ranked 34th in most population and has just 33.6 percent receiving the immunization series.
Ferry is ranked 36th in most population and has just 35.6 percent receiving the immunization series.
Garfield is ranked last out of the 39 counties and has just 30.3 percent receiving the immunization series.
Fortunately for these smaller counties, Washington health agencies, notably the Vaccine Advisory Committee and the Washington Vaccine Association, have their CDC Big Brother buddies’ Vaccination in Rural America Special Report to both guide and inspire them. It’s filled with nineteen pages of vaccination strategies for rural America that would make any Big Pharma marketing department proud. (Sarcasm included for free).
The Report’s overview should be enticing to the health department heads in our small counties:
This State of Vaccine Confidence Insights Report emphasizes major themes influencing general vaccine confidence and uptake among rural populations in the United States between 2017-2023, with a particular focus on COVID-19 vaccination.
Themes with the potential to impact vaccine confidence and demand:
Theme 1: Residents in rural parts of the United States have concerns about vaccine safety, long term side effects, effectiveness, and necessity.
Theme 2: Differences exist in vaccine access and vaccine confidence between rural areas and suburban and urban areas.
Theme 3: Lack of government trust and the politicization of science may have contributed to lower vaccine uptake in rural areas. However, community outreach and utilizing trusted messengers can and has increased vaccine confidence in rural America.
Ways public health and partners can take action to improve vaccine confidence and demand:
Offer additional services at vaccination sites to increase comfort of individuals seeking vaccination, such as multilingual support, vaccine counseling, and family-friendly services. Provide opportunities for community members to ask questions and voice their concerns.
Offer channels for direct communication, such as helplines, email, or in-person meetings, where trained professionals can provide personalized information and address specific worries.
Share multilingual messages that present the benefits of youth vaccination against COVID-19, including protection from severe illness or hospitalization and the ability to safely participate in childcare, school, sports, and other group activities. When possible, provide safety information and ways to have questions answered as part of this messaging approach.
Ensure all messaging acknowledges and recognizes the diversity of rural populations and does not falsely label rural populations as monolithic.
Complete need-based assessments and rapid community assessments to identify and address specific barriers in rural communities.
Create community-based networks to increase vaccine access, such as providing vaccine appointments after traditional work hours.
To build trust with rural residents, engage with trusted community leaders, gather community input on questions and concerns, and work to prioritize and address them.
Encourage state and local health departments, community pharmacists, and other local trusted messengers to promote vaccine messaging in communities where they are the preferred trusted messenger over federal agencies.
Utilize nontraditional sites like school-based health centers and mobile clinics to bridge the vaccination access gap in rural areas.
Address inaccurate health information about vaccine safety and effectiveness by leveraging health care professionals, public health departments, libraries, and other local institutions to answer consumer questions and provide informative resources.
Provide support and guidance on managing common side effects and reassure the community that any adverse events are being closely monitored and addressed.
Continue to implement evidence-based vaccination-promoting interventions endorsed by the Community Preventive Services Task Force.
The best details for the state health agencies to look at for this marketing advice falls on page eleven, which first addresses the problem of vaccine hesitancy in rural areas.
Vaccine hesitancy in rural populations
A qualitative study exploring rural Americans’ COVID-19 vaccine perceptions found that vaccine hesitant adults were more likely to trust local sources of health information such as healthcare providers, pharmacists, and county government officials. [footnote 43]
Vaccine uptake and confidence can be influenced by an individual or community’s values, beliefs, and sense of identity, including political affiliation.[footnotes 44,45,46,47] As such, it is important to engage with rural communities in a manner that recognizes and resonates with their cultural and social context.
More than 600 vaccine-related bills have been introduced so far in 2023, eclipsing the total number of bills introduced in 2022 according to the National Conference of State Legislatures.[48] Many states are considering legislation that would prohibit or curtail COVID-19 vaccine requirements as well as routine vaccine requirements imposed by schools, employers, and other entities.[49]
The rest of the page provides case histories for Washington’s health agencies to follow:
Strategies that have worked to promote vaccine uptake in rural populations
In New York, the University of Rochester formed the Finger Lakes Rural Immunization Initiative, a 16-month project funded by CDC to increase vaccine awareness, knowledge, and acceptance in rural areas by engaging trusted messengers. These efforts resulted in an interactive workshop, interventional toolkit, and stakeholder forum designed to empower trusted messengers and foster community collaboration. Among the trusted messengers who were surveyed following their workshop participation, 45% reported that their patients were more likely to get vaccinated and 29% believed that their patients became vaccinated as a result of the conversational strategies from the workshop.
A study measuring the effectiveness of an HPV vaccination intervention in a rural medical clinic found healthcare team training, education materials, and technology-based vaccine appointment reminders resulted in fewer missed vaccination appointments.[5]
Locations that were well-stocked, efficient, and offered easy access saw positive feedback and support from the rural communities where they were administering the vaccines.[50,51] Consumers in low socioeconomic rural communities were more supportive of clinics and vaccine drives that offered vaccines for free.[40,52]
Homebound consumers in rural counties stated their willingness to receive vaccines if they had the option of at-home administration.
Rural communities in some areas provided mobile vaccine clinics and incentives to reach consumers who desired COVID-19 and influenza vaccines but did not have access otherwise.[53] Trusted messengers and health care professionals were used to address questions about vaccine safety, effectiveness, and misinformation for rural consumers.[54]
Local health departments and other health care professionals posted vaccine facts, and vaccine clinic locations on social media to inform their communities about the vaccines’ safety, efficacy and availability.[55,56] Page: 12 State of Vaccine Confidence Insights Report | September 25, 2023
Research indicates that rural residents might trust community pharmacists for health information and vaccine administration due to a number of factors, such as convenience and connectedness to the communities they serve.[43] Consumers also believe trusted messengers play a large role in encouraging adults in rural America to receive the COVID-19 vaccine.
If you live in any of the smaller counties, you are now more informed and warned about the nudging techniques that your local health departments may use.
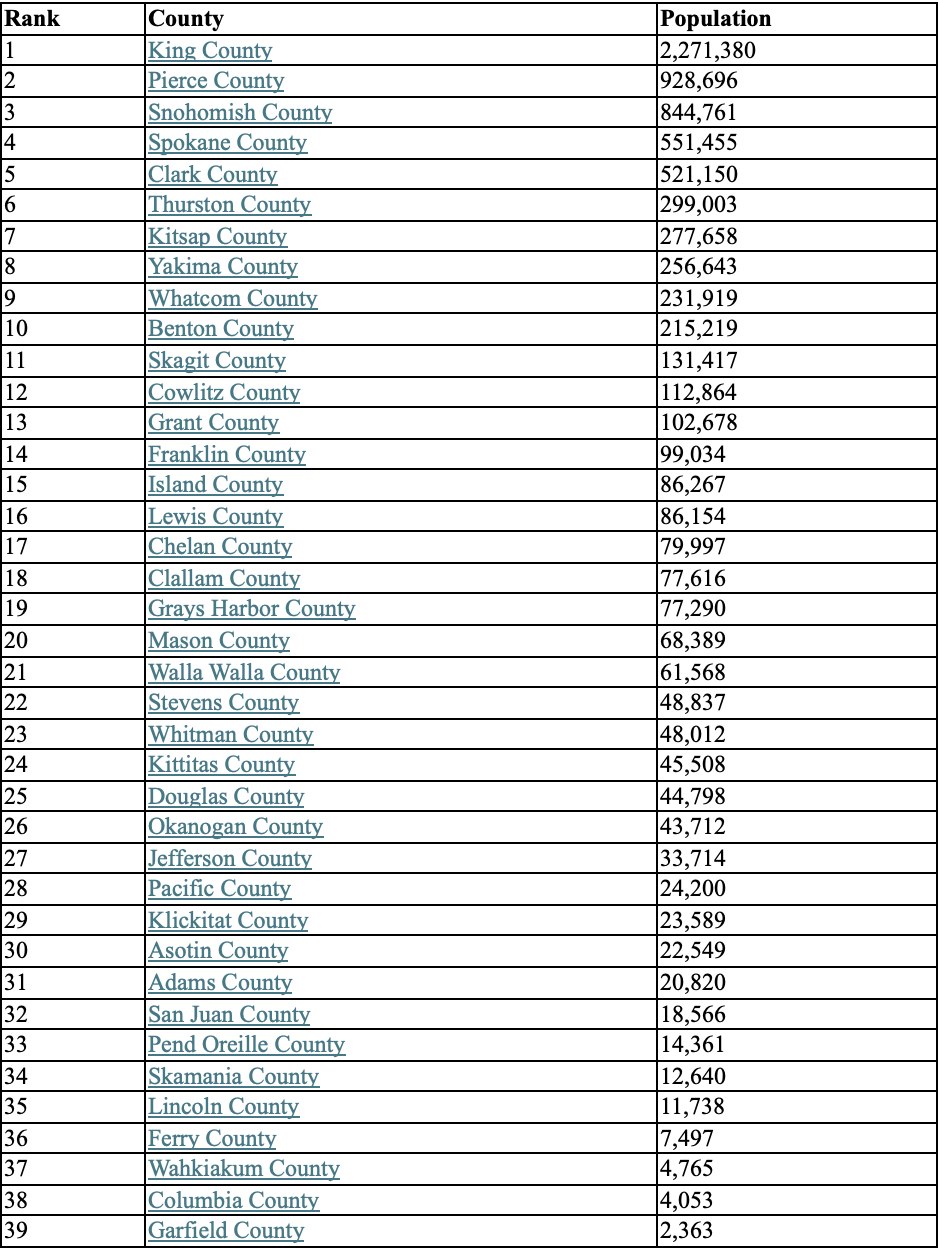
For reference, below is Washington’s population ranking by county.
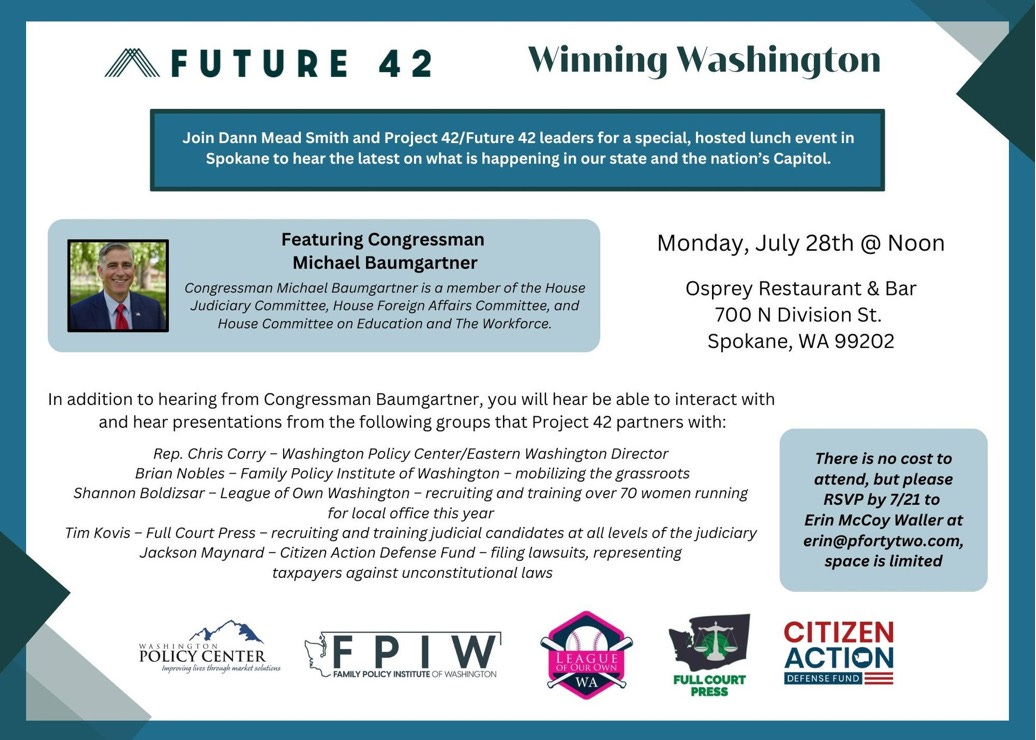
An Event: Spokane, July 28 at noon
Lunch Event by Future 42 on Winning Washington with Congressman Michael Baumgartner
Sponsored by: Family Policy Institute of Washington (our partner) and others.
For some irony:
With regards to the data on rural covid vaxx rates, are those data points for the full series, all boosters or just the initial vaxxes?
This is the Firefighter Terminated by Seattle for the Vaccine Mandate. Contact me with a PM and we can set up an interview. Thanks for offering to help get our story out.